In 1957, the first results of the Framingham Heart Study were published [1]. It was (or I should say, is, as it’s still ongoing) an epidemiological study that sought to find out risk factors for cardiovascular disease. The study is named after the city of Framingham, Massachusetts, in the United States. A total of 5,209 residents of the city between the age of 30 and 62 were recruited. Various data of this group of people (cohort) was gathered over time to discover these risk factors. In their milestone publication, they identified three risk factors for cardiovascular disease: hypertension, obesity, and hypercholesterolemia (high cholesterol levels).
For the purpose of this article, we’ll focus on cholesterol. Before I get to the effect anabolic steroids have on HDL cholesterol, I’ll first provide some more background.
A quick glance at the relation between cardiovascular disease and LDL and HDL cholesterol
After these initial findings of the Framingham Heart Study, the role cholesterol plays in the development of cardiovascular disease risk has been further refined. An early step forward in this area of research was the division of cholesterol into low-density lipoprotein (LDL) cholesterol and high-density lipoprotein (HDL) cholesterol and their respective contributions to cardiovascular disease risk. These two cholesterol fractions are also known to the lay public as “bad” and “good” cholesterol, respectively.
High LDL cholesterol was found to be associated with an increased risk of cardiovascular disease. After decades of research, a plethora of evidence has firmly established this association to be causal [2]. Indeed, LDL-lowering therapy, for example by the use of statins, is a cornerstone of dyslipidemia treatment. The association between HDL cholesterol and cardiovascular disease risk is opposite that of LDL cholesterol: high HDL cholesterol has been found to be associated with a decreased risk of cardiovascular disease. Epidemiologic studies find a decreased cardiovascular risk of approximately 2–3 % for every 1 mg/dL increase in HDL cholesterol [3].
Contrary to LDL cholesterol, however, there doesn’t appear to be a direct causal link between HDL cholesterol levels and cardiovascular disease risk [4]. Human genetic studies, in which certain gene mutations which lead to higher or lower HDL cholesterol levels, didn’t clearly demonstrate an association with cardiovascular disease risk. This would’ve been expected if there was a direct causal link. The disconnect between HDL cholesterol levels and cardiovascular disease risk perhaps became most painfully evident in clinical drug trials. A handful of drugs have been developed (or already existed) that raise HDL cholesterol levels quite significantly, but fail to reduce mortality or the incidence of cardiovascular events, such as stroke or myocardial infarction [5]. This also includes the use of over the counter supplements, such as niacin [5, 6].
Anabolic steroids decrease HDL cholesterol
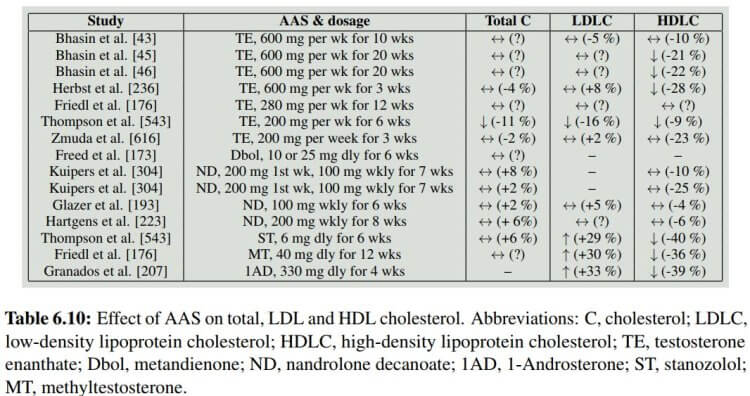
So now you’re up to speed a bit with the relation between cardiovascular disease and LDL and HDL cholesterol. Several interventional trials have looked at the effect of anabolic steroid use on cholesterol. I’ve made a little summary of these studies in Book on Steroids that I show here in the table below. While not all studies found a statistically significant decrease in HDL cholesterol (↔️), many do and overall it just unequivocally shows a decrease. This is particularly true for oral anabolic steroids which appear to have the largest effect on HDL cholesterol.
In one trial, by Bhasin’s group [11], graded dosages of testosterone were administered (25, 50 125, 300, and 600 mg testosterone enanthate weekly). The authors could therefore evaluate whether there was a dose-response relationship between testosterone dosage and HDL cholesterol—and there was. They found a moderate inverse relationship (r = -0.40) between testosterone levels and HDL cholesterol. Thus, at least up to somewhere between 300 to 600 mg weekly, the higher the dosage, the larger the decrease in HDL cholesterol.
In a recent trial, 100 anabolic steroid users were followed over time while they self-administered AAS. Mean dosage, based on label information, was 898 mg per week, thus making their AAS cycle quite representative of common usage by bodybuilders. Measurements were taken before, during, as well as 3 months after the end of their cycle and 1 year after the start of their cycle. HDL cholesterol decreased by 0.4 mmol/L (from 1.2 to 0.8) during use. Which is a substantial decrease. Values had returned to baseline 3 months after cessation of AAS use.
Why do anabolic steroids decrease HDL cholesterol?
Anabolic steroids are thought to decrease HDL cholesterol by increasing the activity of an enzyme called hepatic lipase [7, 8, 9, 10]. It’s an enzyme that’s mainly produced by the liver. As it’s a lipase, it catalyzes hydrolysis reactions on lipids. More specifically, it cleaves off fatty acids from triacylglycerol (triglyceride) and phospholipids from lipoprotein particles, such as HDL cholesterol. By hydrolyzing triacylglycerol and phospholipids from HDL cholesterol, it reduces these particles in size. These smaller particles are catabolized at a higher rate [12].
Thompson et al. looked at these HDL cholesterol subfractions that differ in size [8]. They measured HDL2 and HDL3 cholesterol levels: the HDL2 cholesterol particles are larger and of a lower density than the HDL3 ones. The participating men received 200 mg testosterone enanthate weekly or 6 mg oral stanozolol (Winstrol) daily for 6 weeks in a crossover design. The results were as follows:
| Value | AAS | Baseline | 6 week |
| HDL (mmol/L) | Stanozolol Testosterone | 1.16 1.11 | 0.70 (-40 %)* 1.01 (-9 %)* |
| HDL2 | Stanozolol Testosterone | 0.36 0.28 | 0.08 (-78 %)* 0.26 (-7 %) |
| HDL3 | Stanozolol Testosterone | 0.80 0.85 | 0.62 (-22 %)* 0.72 (-15 %)* |
As can be seen, the largest relative decrease was observed in the larger HDL2 fraction as a result of stanozolol treatment. In contrast, testosterone showed no statistically significant decrease in the HDL2 fraction, but did so in the smaller HDL3 fraction. It’s not completely clear what causes the decrease in this fraction.
Bodybuilders were randomized to receive 200 mg nandrolone decanoate weekly or a placebo [13]. No statistically significant changes in total cholesterol, LDL cholesterol, and HDL cholesterol were found. Similarly, no significant changes were found in the HDL2 and HDL3 cholesterol subfractions. Notably, within the same publication, the authors also report about a study in which they followed a group of strength athletes that was self-administering anabolic steroids. Various compounds in various dosages were used, but it’s worth highlighting that most of them also included an oral anabolic steroid (mostly stanozolol). Herein, HDL cholesterol took a nosedive: from 1.08 mmol/L to 0.43 mmol/L after 8 weeks. The HDL2 cholesterol subfraction decreased from 0.21 to 0.05, and the HDL3 cholesterol subfraction decreased from 0.87 to 0.40 mmol/L.
Effect of anabolic steroids on HDL cholesterol function
Given the disconnect between a drug’s effect on HDL cholesterol levels and cardiovascular disease risk, research started to focus on HDL cholesterol function. HDL cholesterol is the center player in a process called reverse cholesterol transport. In atherosclerosis, cholesterol accumulates in cells from the immune system (macrophages) and in the smooth muscle cells that encircle the blood vessels [14]. These cells, in turn, become so-called foam cells, which marks the starting point of atherosclerosis. HDL cholesterol particles are able to collect cholesterol from these cells—cholesterol efflux. The efflux of cholesterol from foam cells into the HDL cholesterol particles is one way through which HDL cholesterol is thought to exert its protective effects on the arteries. The collected HDL cholesterol can then be returned to the liver, which incorporates it into the bile and can then be secreted into the feces. Similarly, HDL cholesterol particles can transfer some of their contents to LDL particles, which can either end up in foam cells again or be taken up by the liver as well.
There are ways of measuring HDL cholesterol efflux capacity, and the current train of thought is that modulating this might actually affect cardiovascular disease risk, contrary to HDL cholesterol levels per se. There are several ways how HDL cholesterol can take up cholesterol from foam cells. One of them involves a transporter called ATP-binding casette transporter A1 (ABCA1), which is thought to be the most important one [15, 16]. Other transporters, such as ABCG1 and scavenger receptor B1, as well as plain diffusion, also contribute.
Let’s have a look at trials that evaluated the impact of anabolic steroid use on HDL cholesterol efflux capacity. In one (noncontrolled) trial, older hypogonadal men were randomized to TRT with or without dutasteride (a 5a-reductase inhibitor) [17]. After 3 months, TRT had successfully restored testosterone levels of these men within the normal range. HDL cholesterol and HDL cholesterol efflux capacity remained unaltered.
Another trial, which was a randomized-controlled trial, applied a slightly different approach [18]. Healthy men, 19–55 years of age, were medically castrated in order to completely suppress their endogenous production. Following this, they either received a placebo, a low-dose TRT, a full replacement TRT, or a full replacement TRT with letrozole—an aromatase inhibitor which thus inhibits the conversion of testosterone to estradiol. HDL cholesterol increased slightly in the placebo and low-dose group, and remained unaltered in the two groups receiving a full replacement dose. Additionally, while a small decrease was found in ABCA1 efflux capacity in the group that also received letrozole, no changes were observed in the other three groups. Because of the small group sizes, it’s possible that a small effect was missed.
What about high dosages? Unfortunately, there’s only one trial which investigated this, and it was cross-sectional in nature (looking at these measurements at just one point in time, which makes drawing conclusions impossible/difficult) []. The researchers compared measurements in a group of AAS users to that of age-matched strength-trained nonusers and sedentary controls. The AAS users were heavy users, having used AAS on average for about 8 years with a mean dosage of (apparently) 2.5 g weekly. The HDL capacity to efflux cholesterol from macrophages was 13 % lower in the AAS users compared to the matched strength-trained nonusers. Again, because of the cross-sectional nature of the trial, it’s hard to say if this was causal.
Conclusion
Anabolic steroids decrease HDL cholesterol, in a dose-dependent fashion, and this appears especially true for oral anabolic steroids which are 17α-alkylated. It’s uncertain how this translates to cardiovascular disease risk, as there’s a disconnect between a drug’s capability to alter HDL cholesterol and its effect on this. The correlation between measured HDL cholesterol levels and cardiovascular disease risk is not a causal one. Researchers think HDL cholesterol efflux capacity might have a better predictive ability as well as being causally related. As such, drugs that impact efflux capacity might, indeed, affect cardiovascular disease risk. The effect of anabolic steroids on this isn’t that clear yet due to scarcity of data—especially in regard to supraphysiological dosages. There’s a hint of data that suggest that it might negatively impact cholesterol efflux capacity. A longitudinal cohort study is likely to answer this question with some more certainty in the future. If HDL cholesterol efflux capacity indeed decreases as a result of anabolic steroid use, this AAS-induced decrease might be detrimental to cardiovascular health.
References
- T. R. Dawber, F. E. Moore, and G. V. Mann. Measuring the risk of coronary heart disease in adult population groups: Ii. coronary heart disease in the framingham study. American Journal of Public Health and the Nations Health, 47(4 Pt 2):4, 1957
- Ference, Brian A., et al. “Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel.” European heart journal 38.32 (2017): 2459-2472.
- Gordon, David J., et al. “High-density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies.” Circulation 79.1 (1989): 8-15.
- Rader, Daniel J., and G. Kees Hovingh. “HDL and cardiovascular disease.” The Lancet 384.9943 (2014): 618-625.
- Keene, Daniel, et al. “Effect on cardiovascular risk of high density lipoprotein targeted drug treatments niacin, fibrates, and CETP inhibitors: meta-analysis of randomised controlled trials including 117 411 patients.” Bmj 349 (2014).
- Schandelmaier, Stefan, et al. “Niacin for primary and secondary prevention of cardiovascular events.” Cochrane Database of Systematic Reviews 6 (2017).
- Friedl, Karl E., et al. “High-density lipoprotein cholesterol is not decreased if an aromatizable androgen is administered.” Metabolism 39.1 (1990): 69-74.
- Thompson, Paul D., et al. “Contrasting effects of testosterone and stanozolol on serum lipoprotein levels.” Jama 261.8 (1989): 1165-1168.
- Zmuda, Joseph M., et al. “The effect of testosterone aromatization on high-density lipoprotein cholesterol level and postheparin lipolytic activity.” Metabolism 42.4 (1993): 446-450.
- Herbst, Karen L., et al. “Testosterone administration to men increases hepatic lipase activity and decreases HDL and LDL size in 3 wk.” American Journal of Physiology-Endocrinology and Metabolism 284.6 (2003): E1112-E1118.
- Singh, Atam B., et al. “The effects of varying doses of T on insulin sensitivity, plasma lipids, apolipoproteins, and C-reactive protein in healthy young men.” The Journal of Clinical Endocrinology & Metabolism 87.1 (2002): 136-143.
- Jin, Weijun, Dawn Marchadier, and Daniel J. Rader. “Lipases and HDL metabolism.” Trends in Endocrinology & Metabolism 13.4 (2002): 174-178.
- Hartgens, F., et al. “Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a).” British journal of sports medicine 38.3 (2004): 253-259.
- Ouimet, Mireille, Tessa J. Barrett, and Edward A. Fisher. “HDL and reverse cholesterol transport: Basic mechanisms and their roles in vascular health and disease.” Circulation research 124.10 (2019): 1505-1518.
- Du, Xian-Ming, et al. “HDL particle size is a critical determinant of ABCA1-mediated macrophage cellular cholesterol export.” Circulation research 116.7 (2015): 1133-1142.
- Adorni, Maria Pia, et al. “The roles of different pathways in the release of cholesterol from macrophages.” Journal of lipid research 48.11 (2007): 2453-2462.
- Rubinow, Katya B., et al. “Testosterone replacement in hypogonadal men alters the HDL proteome but not HDL cholesterol efflux capacity.” Journal of lipid research 53.7 (2012): 1376-1383.
- Rubinow, Katya B., et al. “Sex steroids mediate discrete effects on HDL cholesterol efflux capacity and particle concentration in healthy men.” Journal of clinical lipidology 12.4 (2018): 1072-1082.
- de Souza, Francis Ribeiro, et al. “Diminished cholesterol efflux mediated by HDL and coronary artery disease in young male anabolic androgenic steroid users.” Atherosclerosis 283 (2019): 100-105.
About the author

Peter Bond is a scientific author with publications on anabolic steroids, the regulation of an important molecular pathway of muscle growth (mTORC1), and the dietary supplement phosphatidic acid. He is the author of several books in Dutch and English, including Book on Steroids and Bond's Dietary Supplements.
Leave a Reply
You must be logged in to post a comment.