Type-IIx
Member
How Exogenous GH Blunts GH Secretagogues' Effects – And How to Deal with It
Author
Cormac J. Mannion (Type-IIx)

Thanks for reading Type-IIx’s Gear, Growth, and Gains Newsletter! This post is public so feel free to share it.
Share
The GH secretagogues fall into two classes, the GH-releasing hormone receptor (GHRH-R) agonists and the GH secretagogue receptor (GHS-R) agonists. GHRH-R agonists include tesamorelin, CJC-1295, and Mod GRF(1-29). GHS-R agonists include ipamorelin, hexarelin, and the small molecule (not peptide) drug, ibutamoren (MK-0677).
Combining these two classes of GH secretagogue creates a superimposition of GH levels in the blood that are "greater than the sum of their parts" – synergistic – as a consequence of increasing the same end-point (GH levels in blood) by different mechanisms. To wit, by the effects on their respective, but different, receptors. In the case of the GHRH-R agonists like tesamorelin, CJC-1295, or Mod GRF(1-29), GH pulses are sped up in a rapid-fire like way, causing more pulses per second, like the rippling-out from above when a hawk dives to snare its prey under the surface of an otherwise placid lake. In the case of the GHS-R agonists like ipamorelin, hexarelin, or ibutamoren (MK-0677), GH pulses are amped up with higher peak GH pulses, causing a sudden GH peak, that burst out of the brain's hypophysis or anterior pituitary like the crescendo of a monstrous ocean wave.
Review
For a review of this topic, refer to the What Are GH Secretagogues Anyway? section of the article Female Use of GH Secretagogues vs. recombinant Human Growth Hormone: The Ultimate Guide

Figure 1: Combined effects of a GHRH-R agonist and a GHS-R agonist on (blood) GH area-under-the-curve. [1].

Figure 2: The GHRP/GHRH/SS/GH/IGF-I Axis Flowchart Diagrams from Symposium 4 – GH Secretagogues vs. Recombinant Human GH PowerPoint presentation. Slide 6 of 30. [2].
First in the loop is somatostatin (SS). Somatostatin is the antimatter to GH – its role is to oppose GH, and to keep GH at bay. To understand this concept we can look at the definitional parts. Somatotropin, or GH; and somatropin, its synthetic 22-K form (rhGH), derive from the Latin root somnus for sleep, when GH is primarily secreted. The suffix '-tropin' is derived from the Greek word tropos meaning to change and biologists and chemists use the '-tropin' suffix to refer to peptides or proteins that stimulate changes to tissues or organs, i.e., growth or hormonal activity. Somatotropin (GH; endogenous) then, refers to "sleep hormone," and Somatropin (rhGH; exogenous) does too1.
Take then, myostatin. The prefix 'myo-' refers to muscle from its Latin root (myo). Myostatin halts or puts the brakes on muscle. The suffix '-statin' comes from the Latin stare which means "to stop." In pharmacology, statins "stop" or inhibit the synthesis of cholesterol. Myostatin stops or inhibits the synthesis of muscle. So, then too, does somatostatin inhibit the synthesis of GH by the pituitary by signaling from the hypothalamus to the pituitary to blunt GH synthesis at its root!
Then, we see the next item – GH!
GH inhibits its own secretion. [2-2]. [6]. The endocrine system and its parts commonly maintain homeostasis by this feature of negative autoregulation. So, like testosterone vis-à-vis its place in the hypothalamo-pituitary gonadal axis (HPGA) – which we colloquially call the HPTA in our world… something that I'm "guilty" of "mislabeling" it as too in spite (truly) of the medical nomenclature designating the HPTA as the hypothalamo-pituitary thyroidal axis... though seeing as I have a pair, there are few things I give a shit less about… Anyway…
Any drug that stimulates the endogenous secretion of GH will then, too, be ensnared by this regulatory loop, meaning, GH will to some degree inhibit or blunt its own (i.e., endogenous) secretion by its secretagogues. Just like how exogenous, supraphysiological testosterone "shuts down" synthesis/secretion of endogenous testosterone.
Well, rhGH inhibits or blunts GH secretion – the endogenous process – which the secretagogues stimulate – indeed their mechanism of action is to stimulate the endogenous synthesis and secretion of GH. [2-3]. [6-1]. [7]. While the GHRH-R agonists increase GH pulse frequency and the GHS-R agonists increase GH pulse amplitude, they combine synergistically to really pulse out GH from the anterior pituitary. [2-4]. RhGH is the same peptide as GH – it has the same effect: to blunt the endogenous pulsatile release of GH by negative autoregulation.
Even physiologic GH pulses during sleep, exercise stress, and short-term starvation (i.e., dieting, caloric restriction) blunt secretagogue efficacy – by diminishing blood GH area-under-the-curve. [6-2]. If taking a nap, training, or dieting levels of GH blunt secretagogue efficacy, you better believe that 4 IU of rhGH does even more so!
So if GH negatively regulates itself endogenously then any drug whose mechanism of action is to stimulate the endogenous secretion of GH, like the secretagogues, then these drugs, the secretagogues, are in the crosshairs of this regulatory loop.
Read More
Author
Cormac J. Mannion (Type-IIx)
Date
Monday, August 4, 2025
Thanks for reading Type-IIx’s Gear, Growth, and Gains Newsletter! This post is public so feel free to share it.
Share
Introduction
Exogenous GH in its recombinant, 22 kilodalton-atom polypeptide form, "bioidentical" to the predominant circulating, evolutionarily conserved, endogenous GH (22-K GH) is referred to as recombinant human GH or rhGH. This peptide needs little introduction: its effects on growth (e.g., muscle, bone, sinew) and metabolism (e.g., shifting from carbohydrate to fat metabolism, increasing blood glucose and free-fatty acids, lipolysis) are not merely established but legendary; and its ubiquity in advanced bodybuilding protocols relates to its time-worn success at reducing fat-mass (especially away from the central abdominal depot) and building lean-mass, promoting a "full, 3-D look." Moreover, its utility for injury prevention by enhancing not merely water and nitrogen but potassium, phosphorus, and other elemental retention in the extracellular space protects the sinews (ligaments, tendons) from chronic wear-and-tear during heavy loading and voluminous training phases.GH Secretagogues
GH secretagogues are peptide drugs (e.g., tesamorelin, ipamorelin) and small molecule drugs (e.g., MK-0677 or ibutamoren) that stimulate the sudden burst-like, pulsatile secretion, of our body's natural GH, from the anterior pituitary, in our brains, that secretes hormones after receiving a signal to from another brain region, the hypothalamus. These bursts, or sudden increases to GH in the blood are called pulses, and they occur during sleep, starvation, and exercise stress, all to prevent protein breakdown primarily.The GH secretagogues fall into two classes, the GH-releasing hormone receptor (GHRH-R) agonists and the GH secretagogue receptor (GHS-R) agonists. GHRH-R agonists include tesamorelin, CJC-1295, and Mod GRF(1-29). GHS-R agonists include ipamorelin, hexarelin, and the small molecule (not peptide) drug, ibutamoren (MK-0677).
Combining these two classes of GH secretagogue creates a superimposition of GH levels in the blood that are "greater than the sum of their parts" – synergistic – as a consequence of increasing the same end-point (GH levels in blood) by different mechanisms. To wit, by the effects on their respective, but different, receptors. In the case of the GHRH-R agonists like tesamorelin, CJC-1295, or Mod GRF(1-29), GH pulses are sped up in a rapid-fire like way, causing more pulses per second, like the rippling-out from above when a hawk dives to snare its prey under the surface of an otherwise placid lake. In the case of the GHS-R agonists like ipamorelin, hexarelin, or ibutamoren (MK-0677), GH pulses are amped up with higher peak GH pulses, causing a sudden GH peak, that burst out of the brain's hypophysis or anterior pituitary like the crescendo of a monstrous ocean wave.
Review
For a review of this topic, refer to the What Are GH Secretagogues Anyway? section of the article Female Use of GH Secretagogues vs. recombinant Human Growth Hormone: The Ultimate Guide
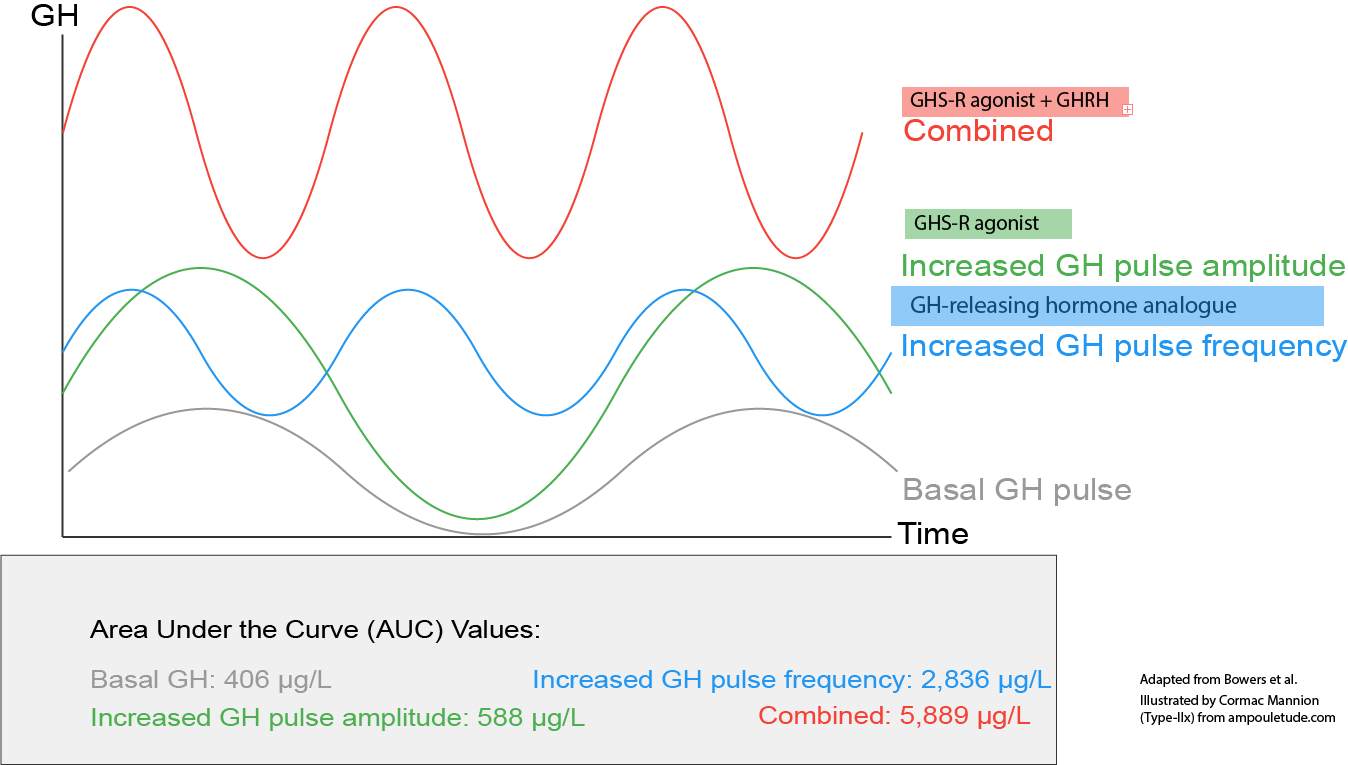
Figure 1: Combined effects of a GHRH-R agonist and a GHS-R agonist on (blood) GH area-under-the-curve. [1].
GHRP/GHRH/SS/GH/IGF-I Axis
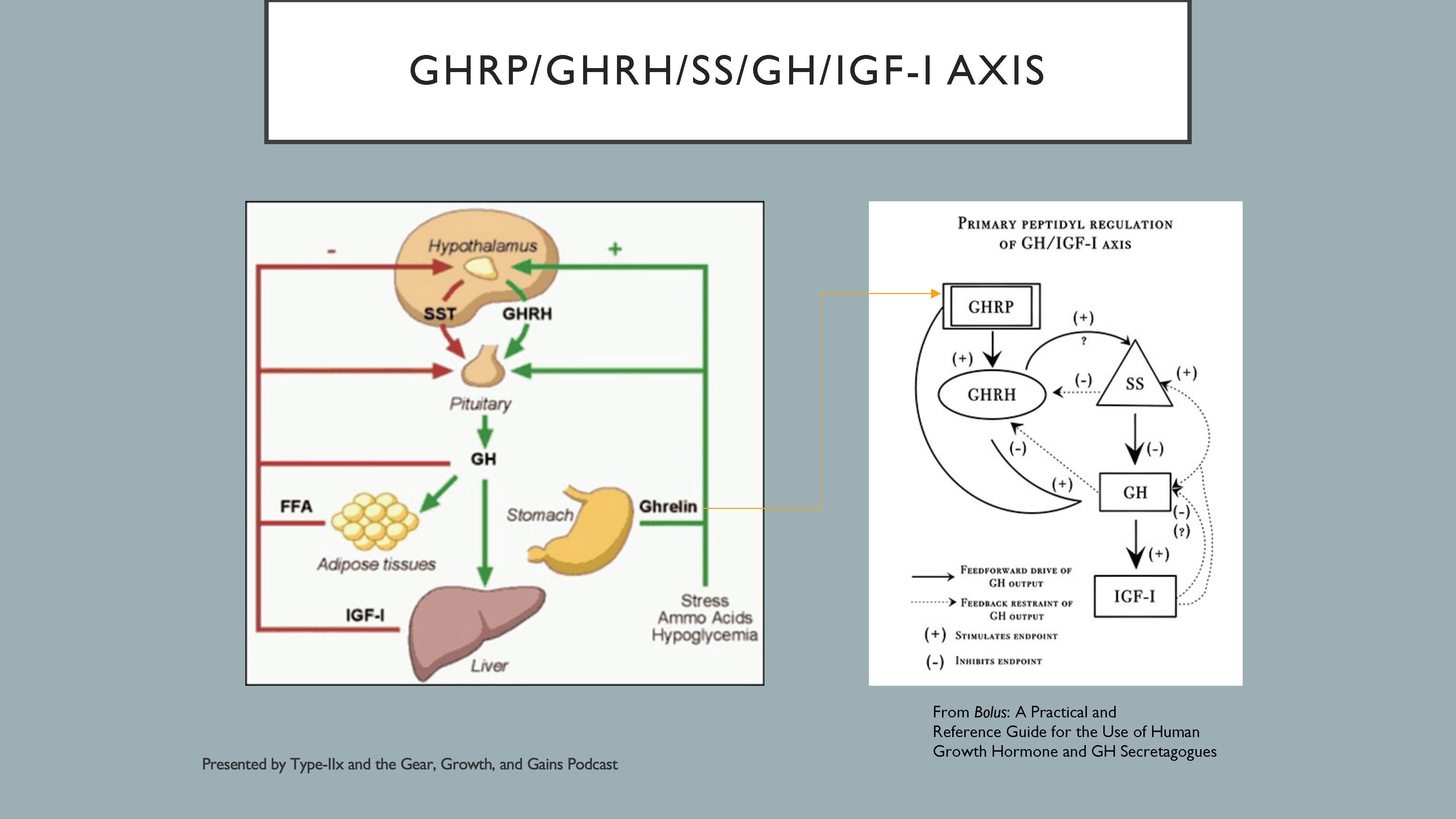
Figure 2: The GHRP/GHRH/SS/GH/IGF-I Axis Flowchart Diagrams from Symposium 4 – GH Secretagogues vs. Recombinant Human GH PowerPoint presentation. Slide 6 of 30. [2].
- The yellow arrow leading from Ghrelin from the flowchart on the left to that on the right links the endogenous ligand to its secretagogue-equivalent activity.
- GHRP is synonymous with Growth Hormone Secretagogue (GHS-R agonist).
- After the 1980 discovery of hexarelin as a potent stimulator of GH secretion, the GHS-R was identified as a novel mechanism to stimulate GH. A 19-year intervening period would follow before its endogenous ligand, ghrelin, was identified! [3]. Probably because it was where you might least expect it… in the stomach. Ghrelin, like GHS-R agonists, makes your stomach grumble and causes an increase in appetite.
- GHRH is synonymous with Growth Hormone-Releasing Hormone (GHRH-R agonist).
In Figure 2, on the left, is a diagram of the endogenous regulation of the GHRP/GHRH/somatostatin/GH/IGF-I axis. [2-1]. The red, negative sign and arrows indicate negative feedback or inhibitory regulation of GH secretion. On the right is a diagram from my book, Bolus, that reorganizes the axis by reference to exogenous secretagogue administration. [4]. The GHRPs – nowadays referred to as the GHS-R agonists, or Ghrelin mimetics since ghrelin, the gut's "hunger hormone" and natural endogenous ligand for the GHS-R – are used to enhance GH drive and pulse amplitude, and the GHRHs are used to enhance GH feedforward and pulse frequency. [5]. [4-1]. The hypothalamus and pituitary glands play critical roles in the regulation of growth (e.g., increased muscle size) and metabolism (e.g., promoting a shift from glucose and protein to fat oxidation) via GH, the regulation of which involves an interplay between Growth Hormone-Releasing Peptide (GHRP) or the Growth Hormone Secretagogue Receptor (GHS-R), Growth Hormone-Releasing Hormone Receptor (GHRH-R), Somatostatin (SS), Growth Hormone (GH), and Insulin-like Growth Factor 1 (IGF-I).
Putting the Brakes on GH
Endogenous Blunting of GH Synthesis and Secretion
So how does all this tie together and relate to the subject of how exogenous GH blunts GH secretagogue effects? To answer this, let's focus our attention on Figure 2, and work our way down the lefthand side of the left diagram, comprising the red arrows that indicate negative regulation, to wit, blunting if not outright blocking.First in the loop is somatostatin (SS). Somatostatin is the antimatter to GH – its role is to oppose GH, and to keep GH at bay. To understand this concept we can look at the definitional parts. Somatotropin, or GH; and somatropin, its synthetic 22-K form (rhGH), derive from the Latin root somnus for sleep, when GH is primarily secreted. The suffix '-tropin' is derived from the Greek word tropos meaning to change and biologists and chemists use the '-tropin' suffix to refer to peptides or proteins that stimulate changes to tissues or organs, i.e., growth or hormonal activity. Somatotropin (GH; endogenous) then, refers to "sleep hormone," and Somatropin (rhGH; exogenous) does too1.
Take then, myostatin. The prefix 'myo-' refers to muscle from its Latin root (myo). Myostatin halts or puts the brakes on muscle. The suffix '-statin' comes from the Latin stare which means "to stop." In pharmacology, statins "stop" or inhibit the synthesis of cholesterol. Myostatin stops or inhibits the synthesis of muscle. So, then too, does somatostatin inhibit the synthesis of GH by the pituitary by signaling from the hypothalamus to the pituitary to blunt GH synthesis at its root!
Then, we see the next item – GH!
GH inhibits its own secretion. [2-2]. [6]. The endocrine system and its parts commonly maintain homeostasis by this feature of negative autoregulation. So, like testosterone vis-à-vis its place in the hypothalamo-pituitary gonadal axis (HPGA) – which we colloquially call the HPTA in our world… something that I'm "guilty" of "mislabeling" it as too in spite (truly) of the medical nomenclature designating the HPTA as the hypothalamo-pituitary thyroidal axis... though seeing as I have a pair, there are few things I give a shit less about… Anyway…
Any drug that stimulates the endogenous secretion of GH will then, too, be ensnared by this regulatory loop, meaning, GH will to some degree inhibit or blunt its own (i.e., endogenous) secretion by its secretagogues. Just like how exogenous, supraphysiological testosterone "shuts down" synthesis/secretion of endogenous testosterone.
Exogenous Blunting of GH Synthesis and Secretion
How Pinning Growth Hormone Blunts GH Secretagogue Efficacy
So, how and when does pinning rhGH factor into all of this?Well, rhGH inhibits or blunts GH secretion – the endogenous process – which the secretagogues stimulate – indeed their mechanism of action is to stimulate the endogenous synthesis and secretion of GH. [2-3]. [6-1]. [7]. While the GHRH-R agonists increase GH pulse frequency and the GHS-R agonists increase GH pulse amplitude, they combine synergistically to really pulse out GH from the anterior pituitary. [2-4]. RhGH is the same peptide as GH – it has the same effect: to blunt the endogenous pulsatile release of GH by negative autoregulation.
Even physiologic GH pulses during sleep, exercise stress, and short-term starvation (i.e., dieting, caloric restriction) blunt secretagogue efficacy – by diminishing blood GH area-under-the-curve. [6-2]. If taking a nap, training, or dieting levels of GH blunt secretagogue efficacy, you better believe that 4 IU of rhGH does even more so!
So if GH negatively regulates itself endogenously then any drug whose mechanism of action is to stimulate the endogenous secretion of GH, like the secretagogues, then these drugs, the secretagogues, are in the crosshairs of this regulatory loop.
Read More


