Most if not everything you need to know in relation to research peptides..
"
Afamelanotide (M-I)
Melanotan One, Scenesse, Afamelanotide (M-I) Dosing:
Light: .5mg
Common: 1mg
Large: 2mg
Melanotan/Afamelanotide is a synthetic version of melanocyte stimulating hormone (a-MSH). Afamelanotide has been shown to induce skin pigmentation through melanogenisis, the production of melanin. Melanin prevents cellular damage in the skin by absorbing, reflecting and refracting light. Melanotan reduces sun damage to UV exposed skin in those with sun allergies.
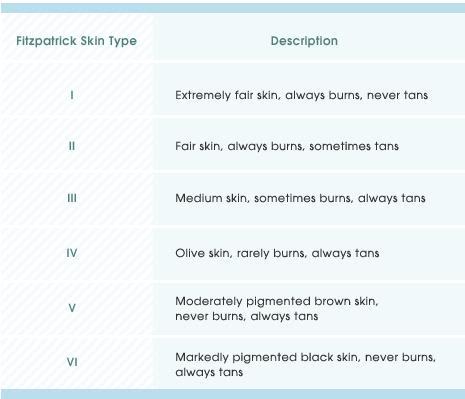
Melanotan favors production of eumelanin (black/brown) over pheomelanin (red/yellow) pigment. Injecting this linear amino acid structure peptide offers super-physiological levels of a-MSH. Learning the majority of secretion of a-MSH comes from the skin as opposed to the pituitary gland was a recent breakthrough in medical science. Those with a Fitzpatrick skin type I-III classification have natural levels of a-MSH that are hardly detectable. The fair skinned can achieve a photoprotective tan with synthetic MSH.
The half-life of Melanotan peptides is very brief. Afamelanotide is being developed in implant form for the ease of use in dermatology. The implant contains 16mg which has a controlled release effecting melanin density for months. Melanotan One is offered in research peptide form (20mg Melanotan One). Peptide Melanotan One gives the user greater control over dosing, however requires a series of injections and expertise. Missing a dose or taking time off is okay. Intermittent therapy, lasting 10 days (skin type III) to 6 months (skin type I) is typical for researchers.
Two amino acids present in the bodies natural a-MSH have been changed in production of Afamelanotide creating a more stable molecule.
Amino acid sequence: Ac-Ser-Tyr-Ser-Nle-Glu-His-D-Phe-Arg-Trp-Gly-Lys-Pro-Val-NH2
Melanotan is still undergoing clinical trials and has not reached approved status. People use on the pretenses and understanding that it is for research purposes only. Users may suffer from slight nausea and flushing after subcutaneous injection; however it is reported to be mild and pass quickly.
Melanotan One is a selective agonist of the MC1R (Melanocortin 1 receptor) and does not have aphrodisiac effects. Melanotan One does not cross the blood brain barrier (BBB). It is for this reason Afamelanotide has continued clinical trials. The fat/weight loss, appetite suppression, libido effects are found in Melanotan 2 and Bremelanotide (PT-141).
Melanotan One is less efficacious than its counterpart Melanotan 2 for achieving a dark tan. Afamelanotide will therefore require 8-10x the dosage to see comparable results. Melanotan One users want minimum side and peripheral effects with a focus on photoprotection.
Administration of Research Melanotan
Safe and controlled administration of Afamelanotide for research is done much like that of Melanotan 2. Melanotan One offered as a peptide in a multi-dose sterile vial is desirable. Implants, nasal sprays and pills are not applicable/efficacious at the present time.
The Melanotan “Cycle”
Allow time before seeing UV exposure. Sunburn is to be avoided.
Example- Skin type II, 180lb male
Day 1-2: .5mg each night
Day 3-6: 1mg when convenient
Day 7-10: 2mg when convenient
Day 11 on forward: begin dosing ~6mg/week
Day 7: 10min sun bed session. (Cover face/genitals/sun damage, use lotion, etc)
Day 9: 10min sun bed session.
Day 11: 15min sun bed session
Dosing According to Skin Type
Fitzpatrick Skin Type I: 1mg-2mg/day. 100mg total may be necessary to achieve desired color. UV exposure after at least 20mg in system
Fitzpatrick Skin Type II: .75mg-1.5mg/day. 60mg should be sufficient to get color. UV exposure after 10-20mg
Fitzpatrick Skin Type III: .5mg-1mg/day. A sunless tan may be realistic here
Fitzpatrick Skin Type IV and beyond: Do not use Melanotan
Melanotan can develop a protective tan in users. A natural tan is developed in response to cell damage caused by UV radiation. Ultraviolet rays penetrate the upper layers of the skin, triggering a-MSH, stimulating melanin production. Melanin deposits act as a natural sunblock at the cellular level. Melanotan injections may offer a way to bring upon a safe, cosmetic tan with less damage.
Melanotan Results
Reconstituting
Swab the stopper of both your M-I vial and the vial of the dilutent (bacteriostatic water) with an alcohol swab.
Take a syringe and draw up your bact water. The amount isn't critical, other than making sure you know exactly how much you have used. The best rule of thumb is choose an amount that will make measuring the final product easy.
Example- 2ml(cc) per 20mg vial of M-I would mean each 10 marks on a U100 insulin syringe would equal 1mg of Melanotan (M-I)
Example- 1ml(cc) per 10mg vial of M-I would mean each 10 marks on a U100 insulin syringe would equal 1mg of Melanotan (M-I)
Avoid shooting the dilutent directly on the lyophilized powder. The powder should almost instantly dissolve. Gently swirl until the liquid is clear if powder did not dissolve upon contact.
Store your unused M-I in the refrigerator. Once reconstituted, the Melanotan should be good for 4-6 weeks in the refrigerator.
Measuring
After successfully reconstituting your peptide, now measure the desired amount out for injection. You will want to use a U100 insulin syringe to draw out your M-I.
Since you know the amount of mg's in your M-I vial, and you also know how much water you have diluted it with, we just divide this out as follows:
Note: 1ml = 1cc = 100 IU's
So we take our number of mg's of Melanotan and we divide that into the amount of dilutent we used.
Example- We used 2cc(ml) of water. We have a 20mg vial of M-I.
From our formula above we know that 1cc = 100 IU's, so we have 200 IU's of water.
We now divide the 200 IU's (the amount of our water) by 20mg (the amount of our M-I)
200 IU / 20mg = 10
This 10 will perfectly correspond with the markings on a U100 insulin syringe. In our example every 10 increments (1/10th of the syringe) on our syringe will equal 1mg of M-I.
Melanotan 2 (MT-II)
Melanotan 2 Dosing:
Light: .5mg
Common: 1mg
Large: 1.5mg
Melanotan 2 (MT-II) is an analog of alpha-melanocyte stimulating hormone (a-MSH). Melanotan 2 comes in the form of a freeze dried (lyophilized) peptide in a sterile multi-use vial.
Melanotan 2 acts on melanocytes to stimulate melanin production. Melanin is the body's natural pigment responsible for your tan.
Melanocortins are a family of peptides beginning with the sequence: His-Phe-Arg-Trp. Melanotan peptides bind to and activate melanocortin receptors (MCRs) which influence pigmentation, inflammation, energy homeostasis, appetite and sexual function. MT-2 MCRs: MC1R, MC3R, MC4R & MC5R.
Melanotan 2 is a smaller and more potent than M-I (which targets MC1R) targeting more receptors. Melanotan 2 has a protective ring-like amino acid structure as compared to a linear peptide such as Melanotan One or Afamelanotide.
What does this mean? The fair skinned CAN achieve a natural tan with synthetic MSH, Melanotan 2. For people with sun allergies these discoveries are life changing. The best defense against skin cancer is a natural tan developed over time. MT-2 was designed to reduce skin cancer rates and be effective as a sunless tanner.
Who uses Melanotan 2? Athletes and fitness enthusiasts choose MT-2 as a lifestyle product to increase tanning efficacy, the aphrodisiac and appetite suppression. MT-2 was dubbed the Barbie drug and has been highlighted in wired. Synthetic melanocortin use helps to attain a tan with the least amount of exposure to harmful ultraviolet radiation (UVR).
Lower skin types on the Fitzpatrick scale are the best candidates for Melanotan 2.
Melanotan treatment stimulates melanin effectively, in particular those with low skin types.
Note: Melanotan is approximately 1,000 times more potent than natural a-MSH and MT-2 has a greater efficacy than M-I.
Disclaimer: Please pursue information regarding the usage of these products from your own research, academic journals, or the research of your in-house scientific team. Products are sold for research purposes are not for human consumption. Remember when you contact these types of stores/
sponsors not to relate the questions or topics to human consumption or they tend not to answer. Always inquire in a research type question.
Melanotan 2 Peptide: Melanotan 2 peptides come in 5mg and 10mg sizes. Photograph at left shows a 5mg and 10mg MT-2 peptide as an example. Peptides within photograph were synthesized by the same laboratory, contain no filler and therefore volume reflects content. All peptides and freeze drying processes are not created equal. Current MT-2 industry standard is the 10mg, 2ml vial size. Trending towards lower doses, freshness, safety, travel and other factors are increasing demand for smaller quantities.
Reconstituted with bacteriostatic water (BW), MT-2 peptide remains potent and preserved. Reconstituting (mixing) your Melanotan 2 peptide is a necessity and will require proper due diligence for results. Nasal sprays, pre-mixed Melanotan 2, pills, oral and loose powder are not often legitimate. There are successful reports of nasal spray experiences, however, they are few and far between as the molecule is larger than the membrane will allow. Enzymes will render the peptide inactive if ingested.
Shipping and Handling: Melanotan peptides are durable and stable. Highlighted in study, the reconstituted MT-2 was shown to be stable at 37 degrees Celsius (98 degrees Fahrenheit) for at least 28 days. Shipping MT-2, even in summer months, is not a problem. Do not pay for cold shipping as it is not a premium. When receiving MT-2 it is recommended to store in the refrigerator.
Mixing: Add BW to the vial when you are ready to begin MT-2 research. View the instructional youtube video on the PT-141 page to see the reconstitution process.
Remove plastic flip top from vial to expose rubber stopper. Needle will pierce the stopper making way inside the vial to turn the white powder into a clear liquid.
Calculator: Add 100 units (1ml) of water to the vial. 1ml/100 units will minimize the volume that you have to inject and will simplify the arithmetic in your MT-2 experiment.
1ml syringe (U100), 1ml BW to reconstitute
Calculations for a desired 0.5mg/500mcg dose:
Step 1= 1ml
Step 2= 10mg MT-II
Step 3= 1ml bact water
Step 4= 500mcg dose
2-3 ticks on your insulin pin (approximately 1/20th of a U100 syringe)
Some prefer to add more dilutent which works fine, take note of the volume increase.
Needles: 29-31 gauge X 1/2", 1 CC (100 unit). That is a typical insulin needle used to mix as well as inject. Use needles one time only. Once your technique perfected, injections are almost painless.
Starting dose: Your first injection should be a very small dose, for example .25mg (250mcg). See how you react. Goal should be to feel nothing. Dose after dinner, before bed. Any dosing chart stating that you should take a high dose (according to your weight) is outdated and potentially dangerous.
Loading dose: Load with 0.5-1mg once a day. People who have used doses in this range generally report getting excellent results. Don’t worry if you miss occasional days. It will not make much difference, focus on the cumulative effects.
Maintenance dose: Maintenance is taking doses less frequently than daily to avoid becoming darker than you want. Yes, that will happen. With enough UVR, you will get much darker than you have even been before. A maintenance dose can help prolong super-physiological photo-protection MT-2 delivers.
UV Radiation: Melanotan is a poor sunless tanner. UV (from sun or a tanning bed) light is necessary to develop a tan. Without it, almost nothing happens. In other words, NO UV = NO TAN. Well, user will pigment depending on skin type.... If you have loaded for a full month and then start UV exposure, you (and your friends) will be astounded by how fast you tan and how dark you get. Moreover, it is advisable to keep areas of your skin that ordinarily get exposure covered up with a towel and/or zinc oxide (nose/lips/face) and let less exposed areas develop pigmentation first. Areas of skin that are typically sun-exposed in your day to day life will respond more readily to the effects of the melanotan peptides.
Fat Loss: The melanocortin (MC) system is a signaling pathway for leptin and insulin. The MC system is important for control of food intake and body weight. MT-2 treatment results in adipocyte lipolysis. MT-2 increases fatty acid oxidation(FAO) in which the MC5R plays a significant role. MT-2 improves insulin sensitivity through stimulating FAO in skeletal muscle tissue. Reduced food intake from the anorectic response of MT-2 is primarily responsible for weight loss.
Watch yourself: Your tan can sneak up on you. A tan generally sets in 3 days after UV rays. Dose and expose yourself gradually to UVR when tanning. Love your skin.
Avoid burning: You are protected from burning mostly by your tan, not the MT-2 peptide. Therefore, don’t overdo the rays at first. Start with only as much UV that you could tolerate without burring before you began Melanotan. It should not take many weeks before you can tolerate hours of strong sun without burning. Truly incredible for those who have never experienced freedom to enjoy the sun.
Continue your regular dosing protocol until you have reached your desired tan and do not want to become darker. Cut injection frequency to once every 2, 3, 4, or even 7 days. Experiment to find the frequency that gives the tan you want.
Storage: Store freeze dried and reconstituted peptides in the refrigerator.
Do you have to inject MT-II?
Yes. The best, most efficient method of administering Melanotan peptides are subcutaneous (subq) injections. Nasal sprays are inconsistent and inefficient. No detectable levels were observed following oral dosing - pills do not work.
Note: There are many things you will need to consider before experimenting with this peptide. Cyclic analogues (MT-II) have a wide range of peripheral effects and systemic control is always going to pose an issue in clinical use. Needless to say, MT-II is not an approved or regulated product. MT-II is legal to buy, possess, etc. Variables such as skin type and individual goals need assessment. Ask for critiques, plans and create a user log during use. Seasoned users are generally more than happy to offer tricks of the trade.
When you start supplementing a-MSH to tan keep in mind that tanning is literally a side effect. The tanning response is, in reality, a physiological repair mechanism to instant UV damage of the skin cells (epidermis/dermis). Melanocyte stimulating hormone is not going to color your skin, it is going to make your own skin create its own tan and that in turn creates protection. If you are looking to be some bronzed beach God with perfectly uniform and specific color then you are better off to going to mystic tan. Redheads, for example, naturally produce a variant form of melanin that is yellowish-red (pheomelanin). Do not expect a brown tan on a ginger body right away.
Know your skin type: Knowing your skin type is just one detail which will help create a user log. There are 10s of thousands of melanotan users worldwide who share the experience. Raise awareness and help others who want to hear success stories, complications and failures.
Am I a good candidate for MT-II?
Melanotan is best suited for the folks with skin types I & II. Prior sun damage, scars, tattoos, freckles, moles, hair color, etc are deciding factors prospective MT-2 users consider. This is a question handled best through asking the audience.
How should I dose MT-II?
Start out small and build up. A typical starting dose is around .25mg and max dose reaching 1mg.
Things to consider: There is no magic pill or formula. Few dermatologists are familiar with Melanotan. The skin is a large, unpredictable organ. Feel comfortable and confident with MT-II before use. Check out as many before and after photos and user logs as you can. A skin type I individual may have to commit months of dedication before dialing in their desired results, be patient.
How much MT-II should I buy and how long will it last?
Skin type I: 30-50mg
Skin type II: 20-30mg
Skin type III: 10mg
Should last entire summer or season
How soon will I begin to see results?
You should notice a change in your skin tone after three weeks. If you have freckles, expect them to get darker before your actual skin color changes.
How long will tan last?
A tan developed using Melanotan 2 lasts much longer than an ordinary tan. A well-tanned person returning from a beach holiday will lose most of the tan in a month if they stop getting sun. But if they had been using Melanotan 2 and continued on maintenance after returning, they would still have most of their tan 3 months later.
Side effects of MT-II?
Possible short-term side effects you should know about, including: nausea, appetite loss, facial flushing and increased libido. These may be noticeable during the first few days of treatment but should taper off.
Dosing an anti-histamine, such as Claritin (Loratadine), works to eliminate sides such as nausea after injecting.
Bremelanotide (PT-141)
Bremelanotide PT-141 Dosing:
Light: .5mg
Common: 1mg
Large: 2mg
Bremelanotide (PT-141) was developed from Melanotan 2 (MT-II), which was tested as a sunless tanning agent. PT-141 is a metabolite of MT-II that lacks the C-terminal amide function-stripping away tanning properties.
Studies have shown bremelanotide to be effective in treating sexual dysfunction in both men (erectile dysfunction or impotence) and women (sexual arousal disorder). PT-141 is the only synthetic aphrodisiac. Unlike Viagra and other related medications (PDE5s), PT-141 does not act upon the vascular system, but directly increases sexual desire via the nervous system (hypothalamus).
Bremelanotide is a melanocortin peptide hormone. PT-141 binds to the melanocortin 4 receptor (MC4R) in particular. Nine out of ten volunteers experienced sexual arousal in trials. The desire is one of the more sought after effects unique to the peptide.
Window of Opportunity:
Although injected (subcutaneously), Bremelanotide has a unique window of opportunity lasting six to 72 hours. In lab trials, female rats exposed to PT-141 immediately began "flirting" with male rats for sex. Postures and movements left no doubt in the male rats minds that they were in the mood.
Women who took part in trials said that they felt a "tingling and a throbbing" along with "a strong desire to have sex." An initial flush occurs post injection, followed by nausea which is dose dependent. For most, effects generally do not take place until a couple hours post injection, peaking around the four hour mark.
Men said PT-141 made them feel "younger and more energetic" as well as sexually interested and aroused. "You're ready to take your pants off and go," said user "a drug that makes you not only able to but eager to."
Dosing: Read as much as possible to gain clarity and align expectations. Gradually dosing increases likelihood for success without sides. A test dose of .25-.5mg on the first attempt is recommended. 1mg, give or take a quarter, is the efficacious dose which yields the most hero stories reported by users.
Bremelanotide PT-141 Peptide:
Bremelanotide in lyophilized form comes in 10mg and 2mg vial sizes (as pictured above -notice the peptide volume -no filler present). Once reconstituted with bacteriostatic water, PT-141 can be stored in the fridge for a couple months and remain potent. Nasal sprays, pre-mixed PT-141, pills and loose powder are not legitimate forms of Bremelanotide. There are successful reports of snorting and nasal spray experiences...however they are few and far between.
Mixing: Bacteriostatic water is used for reconstitution.
Example- 1ml(cc) bacteriostatic water per 10mg PT-141 vial equates to a 1mg dose approximately each 10 units on a U100 insulin syringe.
Example- 1ml(cc) bacteriostatic water per 2mg PT-141 vial equates to a 1mg dose approximately every 50 units on a U100 insulin syringe.
Recommended strategy for mixing and dosing would be to reconstitute with the volume that yields a .1ml injection.
Example- 1ml(cc) bacteriostatic water per 10mg PT-141 vial equates to a 1mg dose approximately each 10 units on a U100 insulin syringe.
Example- .2ml(cc) bacteriostatic water per 2mg PT-141 vial equates to a 1mg dose approximately every 10 units on a U100 insulin syringe.
Human Growth Hormone (HGH)
Human Growth Hormone (HGH) Dosing:
Month 1: HGH 2 IU one injection every other day
Months 2-4: HGH 3 IU one injection five days a week
Months 5-6: HGH 4 IU one injection five days a week
4-6 month cycles are optimal, year round if you are over age 35.
Human Growth Hormone (rHGH, HGH, or GH) is a protein molecule consisting of 191 amino acids. Genetically engineered recombinant human growth hormone is completely identical to the growth hormone made by the human pituitary gland. Researchers have proven growth hormone therapy can reverse the biological effects of aging. HGH is widely appreciated for aesthetics, not necessarily as a performance enhancer.
HGH is released in pulses that take place during the day. Growth hormone is rapidly converted in the liver to its powerful growth promoting metabolite, Insulin like Growth Factor. IGF-1 is measured in the blood to determine the level of growth hormone secretion. Most of the beneficial effects of human growth hormone are directly attributable to IGF-1. Growth hormone replacement/stimulation is the most effective therapy to reverse the effects of aging.
At age 30 people have people have spent most of their lives with relatively high levels of HGH. HGH is responsible for growth during childhood as well as for repair and regeneration of tissue. By the time we are 30 our bodies no longer naturally produce enough GH to handle the damage that is taking place. As this continues, we age. Increasing HGH in our bodies, we can slow, or even reverse many of the manifestations of aging.
What HGH can do:
* Reduce excess body fat, especially abdominal fat. (The reduction of abdominal fat is the single most profound effect of HGH replacement in many people)
* Decrease in the waist to hip ratio. (Meaning fat is removed primarily from around the waist where it is associated with a high risk of coronary disease)
* Increase muscle mass. (and physical strength if combined with moderate exercise)
* Reduce wrinkling of the skin and some other effects of skin aging. (Compliments can be Melanotan and MT-II)
* Re-grow certain internal organs that have atrophied with age.
* Increase bone density.
* Strengthen the immune system.
* Enhanced feeling of well being.
* Reverse cognitive decline.
* Stimulate production of the bone marrow cells that produce red blood cells.
* Reduce the probability that you will spend the last years of your life in a nursing home.
* HGH slows the progression of cardiovascular disease, and reduces the risk of death from cardiovascular disease, in individuals with natural growth hormone levels that are below average for the age of the individual. HGH can also slow the progression of cardiovascular disease by improving one's cholesterol profile. There is increasing evidence over the past year or two that maintaining healthy growth hormone levels results in a stronger heart. Individuals with low growth hormone levels have an overall increased risk of death due to cardiovascular disease. Low growth hormone levels cause a particularly large increase in the risk of stroke as compared with individuals receiving growth hormone replacement.
HGH takes several weeks to months of use benefit from its effects. There are a number of substances that increase the natural secretion of HGH. Some of them are amino acids. The relationship of certain amino acids to growth hormone is complex and varies greatly among different individuals and among individuals of different ages. All absolute and universal statements made about this subject are clearly false.
HGH is a peptide that comes in the form of lyophilized powder. Any other form that you see advertised or run across is likely NOT the real deal. The only way to administer true HGH is by sub-q or intramuscular injection. Be aware that HGH is not anabolic by itself. Careful measures need to be in place during reconstitution.
Reconstituting common HGH, one vial contains powdered freeze-dried HGH and the other vial contains sterile water with a bacteriostatic preservative. When the user is ready to begin, a certain amount of the sterile water is drawn out of the second vial (with a needle and syringe) and injected into the first vial to dissolve the powdered HGH. The solution is then ready for injection. The unused portion is to be kept refrigerated. Use reconstituted HGH within 3 or 4 weeks.
HGH peptide is dissolved by the user because HGH powder is much more durable. The dissolved HGH is very susceptible to being attacked by bacteria and degraded by enzymes. HGH is normally refrigerated, but if HGH powder is is left at room temperature for a few hours, no harm is done as long as the room is not too warm. Sterile powdered HGH can even be left in a cool room for days or weeks, but this is not a good idea. Even the powdered HGH can deteriorate if the temperature rises slightly above normal room temperature for any significant period of time.
The best way to begin HGH is to start with a low dose and ease your way into higher doses. This will allow you to avoid (or at least minimize) many of the more common sides of HGH such as bloating and joint pain. Most can tolerate 1-2 IU per day with few sides. HGH administration should be done on an empty stomach as fats and carbohydrates blunt release. Natural production of GH is 1 IU, give or take a half. For results in athletes the dosing should attempt to duplicate how the body releases the hormone naturally. Learning how much and when to best dose is very individual. My apologies for the dosing chart above.
For bodybuilders growth hormone is best taken in conjunction with insulin, anabolics/androgens, and thyroid hormone. Insulin is extremely effective with HGH as the injections cause a down regulation of insulin sensitivity in the body.
Half life of HGH is 2 hours when injected sub-q with a four hour period which there is a suppression of naturally produced GH. Intramuscular injections shorten the half life. Subcutaneous injections over the long term can lead to spot reduction. Whether or not HGH has any localized benefit from IM injection is unknown, but speculated.
HGH is tightly regulated by the FDA, but HGH is not a controlled substance on the federal level in the United States.
Insulin-like Growth Factor (Long-R3-IGF-1)
IGF-1 (Long R3 IGF-1) Dosing:
Light: 20 mcg
Common: 40 mcg
Large: 80 mcg
IGF-1 is injected post work out (PWO) or in the AM on non workout days for 4-6 week intervals
Insulin-like Growth Factor (Long-R3-IGF-1), an 83 amino acid analog of IGF-1 is a highly anabolic hormone released primarily in the liver with the stimulus of growth hormone (HGH).
Freeze dried (lyophilized) IGF-1 (in powder state) should be stored in the freezer (-18 degrees celsius).
Each Long r3 IGF-1 kit contains:
* 1000mcg of lyophilized Long R3 IGF-1
* 2 mls of 0.6% Acetic Acid (AA)
* 30ml Sodium Chloride (NaCL) as buffer
Dilute the IGF-1 with 2mls of Acetic Acid. Assuming (*DO NOT ASSUME*) AA will yield the correct pH balance of your research peptide.
Note: This creates a concentration of 500mcg/ml. So each 1/10 of a ML is 50mcg’s.
Draw the desired amount of IGF in to a syringe. Desired amount should be the approx dose you want to take.
Example- 2mls AA used to reconstitute IGF-1 1mg vial means 5 units on a U100 insulin syringe would equal 25mcg IGF-1
Pre-load your syringes at 5iu (25mcg IGF-1). Divide your IGF-1 into 20 syringes to move to the freezer for storage.
Thaw prior to administration. Draw from your NaCL after thawed to fill the remainder of your syringe with the buffer (up to 1ml typically).
Administer your test subject intramuscularly (IM) post workout. IGF-1 does not need to be bilaterally or in the muscle trained.
Unknown whether injecting IGF-1 to increase muscle growth is efficacious. Many believe in the value of IGF-1.
Growth Hormone Releasing Peptide (GHRP-6)
GHRP-6 (Growth Hormone Releasing Peptide) Dosing:
Light: 50mcg
Common: 100mcg
Large: 150mcg
Growth Hormone Releasing Peptide (GHRP-6) is a peptide in the growth factor family composed of six amino acids. It has strong effect on the release of Human Growth Hormone (HGH). Dosed at night for anti-aging purposes and multiple times throughout the day for anabolism. GHRP is often used in conjunction with GHRH CJC-1295 to amplify GH pulse. GHRP-6 peptide is typically offered in 5mg vials.
GHRP can be used effectively in the treatment of GH deficiency. Main use is to promote food intake by stimulating hunger and aid in energy metabolism. The major side effect being a significant increase in appetite due to a stimulating the release of Ghrelin, a hormone released naturally in the lining of the stomach and increases hunger and gastric emptying.
Benefits of increased HGH levels through GHRP-6 stimulation include: an increase in strength, muscle mass and body fat loss, rejuvenation and strengthening of joints, connective tissue and bone mass. Enhanced HGH secretion also leads to the liver secreting more IGF-1, which is thought to be the primary anabolic mechanism of action for Growth Hormone.
Mixing: Bacteriostatic water is used for reconstitution. When diluted, peptide lasts a very long time when left alone in the refrigerator (months).
Example- 2.5ml(cc) bacteriostatic water per 5mg GHRP vial equates to a 100mcg dose approximately each 2-3 marks on a U100 insulin syringe.
Example- 5ml(cc) bacteriostatic water per 5mg GHRP vial equates to a 100mcg dose approximately every 5 marks on a U100 insulin syringe.
Dosing: The saturation dose of GHRP-6 has been determined to be around 100mcg
5mg GHRP = 5,000mcg
5,000mcg/100mcg = 50 100mcg GHRP doses per 5mg
GHRP-6 may be the most cost effective secretalogue available today.
Growth Hormone Releasing Hormone CJC-1295
CJC-1295 Dosing:
Light: 50 mcg
Common: 100 mcg
Large: 250 mcg
Growth Hormone Releasing Hormone (GHRH) CJC-1295 is a synthetic secretalogue, when injected stimulates HGH release from the hypothalamus. Dosing GHRH once at night for anti-aging purposes and multiple injections (1-3x) for anabolism. CJC-1295 has the ability to make the body produce its own GH as compared to using synthetic HGH. GHRP-6 use in conjunction with CJC-1295 is synergistic, amplifying the GH pulse considerably.
CJC-1295 is typically found in 2mg vials. Reconstitute with BW. Inject subcutaneously.
Researchers report positive effects much like that of HGH. Particularly energy, quality sleep, fat loss/metabolism, improved skin quality, pumps in the gym.
Most common desirable form to find and research with CJC-1295 (Growth Hormone Releasing Factor) is a modified GRF (1-29), lacking the DAC (drug affinity complex). This GHRH has a short half life. Post injection flush is common."
Reconstitution
Peptides come in the form of lyophilized (freeze dried) powder. The amount of powder/product is stated in International Units (IU's) or in Milligrams (mg)
Melanotan peptides (Afamelanotide & Melanotan 2), PT-141, CJC-1295 & GHRPs (GRHP-2 & GHRP-6), HGH, GH fragments, et cetera use Bacteriostatic Water (BW). Bacteriostatic Water for injection, USP is a sterile, nonpyrogenic preparation of water for injection containing 0.9% of benzyl alcohol added as a bacteriostatic preservative. It is supplied in a multiple-dose container from which repeated withdrawals may be made to dilute or dissolve drugs for injection. The pH is 5.7 (4.5 to 7.0)
For IGF use an acetic acid solution (.6%) which is 7 parts distilled water and 1 part vinegar. You must filter the distilled water and white wine vinegar through a sterile 20 micron syringe filter before use. NaCl is used to buffer the injection.
1.) Take an alcohol swab to the stopper of both your peptide vial and the vial of the dilutent.
2.) Draw your preferred dilutent (BW) with a 1cc syringe. Choose an amount that will make measuring the final product simple.
1ml(cc) per 10 mg vial of Melanotan would mean each 10 tick marks on a U100 slin syringe would equal 1mg of Melanotan
1ml(cc) per 10 IU vial of HGH would mean each 10 tick marks on a U100 slin syringe would equal 1 IU of HGH
3.) Take the syringe with the dilutent and push it into the vial of lyophilized powder letting the dilutent dissolve the peptide. Many (not all) peptides are sealed with vacuum pressure, be careful.
4.) After dilutent has been added to the vial, gentling swirl the vial until the lyophilized powder has dissolved and you are left with a clear liquid. The peptide is now ready for use.
5.) Store your now reconstituted peptide in the refrigerator.
Measurement
After successfully reconstituting your peptide, measure the desired amount out for injection. Use a U100 insulin syringe to draw out and inject your product.
Since you know the amount of IU's/MG's in your vial, we divide this out as follows:
You will need to know the following to be successful: 1ml = 1cc = 100 IU's
We take our dose from the label of the dry lyophilized powder and we divide that into the amount of dilutent used.
example- We used 1cc(ml) of water. We have a 10 IU vial of HGH.
From our formula above we know that 1cc = 100 IU's, so we have 100 IU's of water.
We now divide the 100 IU's (the amount of our water) by 10 IU's (the amount of our HGH)
100 IU / 10 IU = 10
This 10 will perfectly correspond with the markings on a U100 insulin syringe. In our example every 10 mark on our syringe will equal 1 IU of HGH. Want to draw out 2 IU's of GH? ....draw out to the 20 mark on the syringe (1/5th of the syringe).
Say you have a 1mg vial and you add 1ML you get
1000mcg/1mL: 10 mcg per IU
1000mcg/2mL: 5 mcg per IU
Say you have a 10mg vial and you add 1ML you get
10mg/1mL: 1 mg per 10 IU
10mg/2mL: .5 mg per 10 IU
Say you have a 20mg vial and you add 1ML you get
20mg/1mL: 2 mg per 10 IU
20mg/2mL: 1 mg per 10 IU
Say you have a 10iu vial and you add 1ML you get
10iu/1mL: 1 iu per 10 IU (on the syringe - 1/10th the product)
10iu/2mL: 1 iu per 20 IU (on the syringe - still 1/10th the product)
Say you have a 5000iu vial and you add 1ML you get
5000iu/1mL: 500iu per 10 IU
5000iu/2mL: 250iu per 10 IU
Recap:
1.) How much actual product you are dealing with (MG or IU)
2.) How much water (dilutent) you are using to add to powder
3.) Divide the amount of water in units by the amount MG/IU.
4.) This result will equal the measurement on your U100 Insulin syringe per unit
5.) Multiply the number you get it step 4 by how many units you want to inject. This is the number to draw to on your syringe
Injection
1. Always wash your hands thoroughly.
2. Load up the syringe.
* Take the protective cover of the needle, top and bottom.
* Pull back the needle plunger to draw in the air equivalent to the dose you will draw.
* Insert the needle into the vial through the center of the rubber stopper.
* Inject the air into the vial. Leave needle in the vial.
* Turn the vial upside down with the needle still inside.
* Pull back the plunger again to the desired dosage mark on your needle.
* Check your needle for any air bubbles, tap the needle so they rise to the top and then push the plunger to remove them.
3. Select the injection site.
* You can inject anywhere on the body where there is a higher fatty layer.
* Always vary the injection site.
* Never inject any bruised, swollen or scarred areas.
4. Clean the injection site.
* Clean a two-inch area of the selected site with an alcohol swab.
* Let the area dry.
5. Actual injection.
* Using the hand you write with, hold the needle over the area you have cleaned.
* With your other hand pinch two to three inches on either side of the area you have cleaned.
* Using a quick motion, insert the needle into the pinched area. The needle should go all the way into the skin.
* Push the needle plunger until all is out of the needle.
* Pull the needle straight out.
* Apply gentle pressure to the site with the alcohol wipe.
* Do not rub the injection site.
How much is a ml, cc, iu?
ml = milliliter. This is a VOLUME measurement. it is 1/1000 of a liter. When talking about water or similar liquids, it is equivalent to one cubic centimeter.
cc = cubic centimeter. This is also a VOLUME measurement. Most syringes measure their capacity in cc's. If you have a 1cc syringe, it will hold 1ml of liquid.
iu = international unit. This is a unit used to measure the activity (that is, the effect) of many vitamins and drugs. For each substance to which this unit applies, there is an international agreement specifying the biological effect expected with a dose of 1 IU. Other quantities of the substance are then expressed as multiples of this standard. This also means that this measurement is not based on sheer volume or weight of the substance, but rather the effect.
mg = milligram. This is a WEIGHT measurement. It is 1/1000 of a gram. the amount of chemical substance is often measured in milligrams. For injectable solutions, this will be reported as a concentration of weight to volume, such as mg/ml (milligrams per milliliter). In the case of orally administered substances, the weight of chemical is labeled, although the actual weight of the pill/capsule may be much higher, because of the use of filler substances. This means that a small pill may be much more potent than a large pill, so don't judge a pill based on its size, but the actual amount of substance for which it is labeled as.
mcg = microgram = 1/1000 of a mg (milligram) There are one thousand micrograms in one milligram.
Conversion factors:
1000 mcg (microgram) = 1 mg (milligram)
1000 mg (milligram) = 1 g (gram)
1000 g (gram) = 1 kg (kilogram)
1000 ml (milliliter) = 1 liter
1ml (water) = 1cc (water)
Q. What is a Peptide?
A. Peptides are cell messengers that nourish, repair, and send neural-messages, which naturally stimulate diminished collagen and other important skin tissues as well as relax repetitive wrinkle-causing facial expressions. Peptides are found in nature, but are lab-enhanced for safety, maximum efficacy and stability.
Peptides are small protein fragments. A peptide molecule is formed by joining two or more amino acids. When the number of amino acids is less than about 50, these molecules are named peptides while larger sequences are referred to as proteins. The amino acids are coupled by a peptide bond, a special linkage in which the nitrogen atom of one amino acid binds to the carboxyl carbon atom of another. Peptides are present in every living cell and possess a variety of biochemical activities. They appear as enzymes, hormones, antibiotics, receptors, etc.
Q. How should the peptide(s) be stored?
A. The lyophilized product should be stored in the refrigerator. Only place in the freezer for long term storage. Peptides can be good for two years or more.
Q: What purity do I need for my experiments?
A. The final purity of a peptide is very important and depends on the type of experimentation you are doing:
• For non-sensitive screening assays crude or >75% is recommended.
• For immunogen grade >85% is recommended.
• For receptor/ligand studies, bio-assay studies, or cell studies >95% is recommended.
• For structural studies >98% is recommended.
Q. What should the peptide(s) be reconstituted (mixed) with?
A. When in doubt reconstitute with Bacteriostatic Water (BW) for Human Growth Hormone (HGH), HCG, PT-141, Melanotan peptides (M-I, MT-II), both GHRHs (CJC-1295, tetra-sub or modified GRF(1-29) and Sermorelin) & GHRPs (GHRP-6, GHRP-2, Hexarelin & Ipamorelin). Sterile water does not contain benzyl alcholol as preservative and should be used within days.
Do not Reuse Needles
The harm you can cause yourself by reusing a needle is much greater than any convenience or cost savings. The tips of needles may become damaged after just one injection. Even though you can't see this damage it's still there - and it may become worse each time you reuse. There are a lot of good reasons not to reuse syringe or pen needles:
The tip of a reused needle can be weakened to the point where it breaks off and gets stuck under your skin.
A reused needle doesn't inject as easily or as cleanly as a new one and can cause pain, bleeding, and bruising.
Studies have shown that there's a link between needle reuse and the appearance of lumps of fatty tissue that can form at an injection site (lipodystrophy).
Thin, fine, high quality needles are designed to be used one time only.")

















