Back in the early 2000s alot of the research chem websites used to offer rhIGF-1, but it never sold well compared to other offerings and nowadays you just dont see it offered as much but its very easy to find manufacturers that will sell you it just use chemicalregister.com to search.
The general concensus over the years was that rhIGF-1 injected would mostly exert its effects at the site of administration, therefore broscientists believed its main use would be for localized growth of specific muscle groups. Bros believed that any economically feasible amount to use would be fully taken up by receptors at the site of administration before it could circulate systematically. This consensus may be partly to blame with its lack of popularity. Some bros ev3n began trying a protocol for localized muscle growth using rhIGF-1 and PGF2a which is a prostaglandin that supposedly can mimic the effect of working the muscle out. I never heard any rave reviews about the protocol.
In contrast to that broscientist belief about rhigf-1 however are studies showing its systematic administration (subcutaneous) to promote endochondral ossification in the long bones of children. IF systematic administration would not work then one would expect it to have no effect on long bone growth as they are most certainly not injecting it directly into the epiphyseal growth plates of these kids. So this flies in the face of broscientists beliefs from times past.
Now lets muddy the waters more. there was and may still be a product out there called Iplex. Now Iplex is a combo product of rhIGF-1 and IGFBP3. Basically they pre-bound the igf-1 to its most abundant natively endogenous binding protein igfbp3. The claim was this made it far more effective than regular rhIGF-1. Some years back i searched and tried very hard to get my hands on some Iplex but was never able to, its very rare and exotic pharma product and may not even be on the market anymore im not sure as ive fallen out of the researching loop.
Malf if you got time to kill you should dredge up some studies that cross compare iplex (igf-1/igfbp3 complex) verse increlex (igf-1)and post them here.
A bit of logic as well: if rhIGF-1 is so effective in and of itself wh3n administered from an exogenous source, why did Insmed make Iplex (igf1/igfbp3) and why did GroPep make Long R3? Solely to have something they can patent?? Or because they could make igf-1 more effective and overcome a perceivable obstacle to its clinical utilization: short half-life?
In order to draw a conclusion on why the RH-IGF-1 wasn't that successful in the early 2000s vs other chems, it'd be great to find out if it was the RH IGF-1 to begin with and besides it's authenticity there's quality and price factors.
Bodybuilding is based on broscience. =) There's no clinical data telling us how to stack Tren and Test, or use HGH at dosages needed to stimulate muscle growth in healthy individuals. So athletes experiment and see if it is worth taking and spend $ on.
"RH IGF-1 has a short half-life"
Terminal half-life averages 5.8 hours in children with severe primary IGFD1 11 16 25 and 19.2 hours in healthy individuals (from drugs dot com on Increlex)
From what I read, if your kid was prescribed RH IGF-1 and you can afford or insurance covers Iplex, then go with Iplex, as it only needs to be injected once daily vs Increlex x 2 times/day. I don't think that injecting something twice a day was ever a problem among bodybuilders.
Iplex can also be beneficial to :
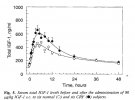
"In addition, the serum half-life of unbound rhIGF-I is shorter when administered to patients with GHIS, who have low serum concentrations of its binding proteins IGFBP-3 and acid-labile subunit (ALS), than when administered to normal volunteers or to the patient with an IGF-I gene deletion (who had normal levels of IGFBP-3). "
I can see the logic behind adding IGFBP-3 to IGF-1 (see above). I can't say the same about IGF-1 LR3, I doubt they were not aware that it's not gonna be bioidentical to any endogenous hormone, antibodies and immunogenicity.
The market was guaranteed to Iplex : all the active components are bioidentical, insurance will cover the costs of the therapy (not many could afford it otherwise), prolly faster approval from FDA. what about IGF-1 LR3? I can assume they were not planning on putting their product in pharmacies.
RS