I take them as separate pills. I actually take a 10mg rosu and split it 4 ways and a 10mg eze and split it in half. The BA is only offered in 180mg so it is split in half. The pills are already so tiny taking all 3 at once is no problem.Do you take them separately or you have a combo pill with those dosage? Here where I live they sell 5mg rosu/10mg ezetemibe I was thinking of splitting those pills but it's really not recommended to split combo pills
MESO-Rx
Anabolic Steroids
Navigation
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
More options
Style variation
Guest viewing is limited
- You have a limited number of page views remaining
- 5 guest views remaining
- Register now to remove this limitation
- Already a member? Click here to login
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Who here is on a statin?
- Thread starter Juicedhead
- Start date
Georgetrenson
Member
Want to chime in, I'm a big fan of throwing in cardarine to help w/ lipids near the end of a cycle when I need a little more lipid support;
I'd def give this a shot and keep using this alternative before I resulting to statins. I know people mention the cancer risk, but this drug is very clean, I'm willing to bet its better for my body as opposed to risking the statin side effects.
Lipid support progression: Niacin+Omega 3+Citrus Bergamot->Cardarine->Statins (stacking each step by step when needed)
I'd def give this a shot and keep using this alternative before I resulting to statins. I know people mention the cancer risk, but this drug is very clean, I'm willing to bet its better for my body as opposed to risking the statin side effects.
Lipid support progression: Niacin+Omega 3+Citrus Bergamot->Cardarine->Statins (stacking each step by step when needed)
egruberman
Member
I'd def give this a shot and keep using this alternative before I resulting to statins. I know people mention the cancer risk, but this drug is very clean, I'm willing to bet its better for my body as opposed to risking the statin side effects.
You're a fool if you believe this.
Lipid support progression: Niacin+Omega 3+Citrus Bergamot->Cardarine->Statins
Please stop giving ill-informed advice.
The evidence on Niacin has been thoroughly established. Not only does it not improve outcomes, it actually makes them worse. See the HPS2-THRIVE trial as well as the AIM-HIGH trial. Those are about a decade old. Since being published there are several other meta-analyses showing the absence of benefit. Most recently, the 2024 Hazen study shows Niacin actually increases risk of MACE: Metabolic product of excess niacin is linked to increased risk of cardiovascular events - Nature Reviews Cardiology
Access to that particular study is paywalled, but there's plenty of detail to be found in medical journalism.
Omega-3 fatty acid is great, anti-inflammatory, but dosing matters. 4g/day of EPA is quite a lot and has potential side effects. The REDUCE-IT Trial showed a significant reduction in MACE, but they were using 4g/day of a very purified form of EPA. There's the JELIS trial conducted in Japan in 2007 showing a reduction in MACE using 2g/day. More recently the 2020 STRENGTH trial using a combo of EPA/DHA did not show an improvement in outcomes.
Citrus Bergamot is a fine supplement that works even better in concert with a statin.
As for cardarine, well, that's a research chemical that never underwent clinical trials. It may yield a benefit, but there's no chance in hell it's superior to a statin in terms of efficacy and safety.
Last edited:
Georgetrenson
Member
Guess my body doesn't work like the people in those trials. When I take the supplements I mentioned, I feel great, when I don't, I feel worse. Everyone's body is different, reading your body is what it all comes down to in the end.
Intuition is paramount to success.
Intuition is paramount to success.
But what do they do for your lipids profile? You might feel great on them, but "feels" is not a solid metric when looking at long-term health outcomes.Guess my body doesn't work like the people in those trials. When I take the supplements I mentioned, I feel great, when I don't, I feel worse. Everyone's body is different, reading your body is what it all comes down to in the end.
Intuition is paramount to success.
Georgetrenson
Member
Theyre good, total cholesterol has always remained under 120 even between blast and cruise as I would adjust the supplements based on anabolic dosage.But what do they do for your lipids profile? You might feel great on them, but "feels" is not a solid metric when looking at long-term health outcomes.
I admit I haven't done extensive enough testing to compare the effects off and on, but I am able to keep LDL and ApoB levels in control w/ year round DHTs, and have not been experiencing the adverse effects mentioned from the research above, so what I'm doing isn't hurting.
For Niacin, I have tested a total cholesterol of around 70 running a cruise dose of test and primo; most absurdly low lipids I've ever seen on bloodwork, I very HIGHLY doubt Niacin is adverse for your health; whenever I feel toxicity from Masteron, I always notice an improvement in well being when I increase my daily dosage of Niacin.
For Cardarine, I think it has an incredible effect on cardiovascular health; when I run it with Anavar I find I can run it for much longer w/ much less adverse effects on cardiovascular performance and overall wellbeing / toxicity. Its a very powerful, efficacious drug, and I personally find the cancer risk worth it.
My goal is to optimize the net effect of my health, focusing on every little detail just leads to confusion and is unnecessary. I understand the issue with going by feel, but in the end my cholesterol has checked out, I wouldn't consider myself blind and misguided w/ the bloodwork I've seen.
Can't tell you enough about the times that studies have contradicted my personal experience w/ things; once I threw science out the door and listened to my body, the process got infinitely better. Intuition is KING.
Last edited:
SenorSuperdrol
Member
Let me start off by saying if your anti statin because of sides, but have done tren your opinion is not qualified for and intelligent conversation
I take rousuvastatin. I’ve experimented with 2.5 a day and 5mg eod. They wield about the same results for me. I also take ezetimbe,
Naturally every study is done on a demographic that won’t represent the typical AAS user. We almost inevitably have the same genetic risks as the general population. We’ll eat better, but through our hormone use we’ll always be hyperlipidemic obviously.
I’d argue the side effect potential is over blown, and not relevant to us. The rhabdo, joint pain, and diabetes is all in individuals that are in poor health. The dosing protocol is 4-8x what can yield great results (2.5mg a day) we arnt getting rhabdo on cycle, and the chance of diabetes with all our tissue as a glucose sink seems unlikely.
I have had great success with my protocol my ldl is always under 80 now and my ratio is less than 3 to 1. I see no reason no to use it. Guys will spend 100’s of dollars on supplements that work 10% as good, it’s nonsensical.
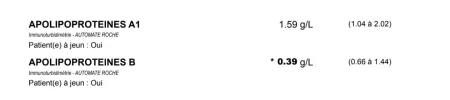
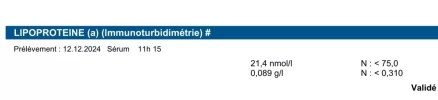
Bloods below are between July and November, on a gram of gear & Drol taken 50-100mg 3x a week on S/B/D days.
I take rousuvastatin. I’ve experimented with 2.5 a day and 5mg eod. They wield about the same results for me. I also take ezetimbe,
Naturally every study is done on a demographic that won’t represent the typical AAS user. We almost inevitably have the same genetic risks as the general population. We’ll eat better, but through our hormone use we’ll always be hyperlipidemic obviously.
I’d argue the side effect potential is over blown, and not relevant to us. The rhabdo, joint pain, and diabetes is all in individuals that are in poor health. The dosing protocol is 4-8x what can yield great results (2.5mg a day) we arnt getting rhabdo on cycle, and the chance of diabetes with all our tissue as a glucose sink seems unlikely.
I have had great success with my protocol my ldl is always under 80 now and my ratio is less than 3 to 1. I see no reason no to use it. Guys will spend 100’s of dollars on supplements that work 10% as good, it’s nonsensical.
Bloods below are between July and November, on a gram of gear & Drol taken 50-100mg 3x a week on S/B/D days.
Attachments

Last edited:
You might look into managing HDL, LDL, and triglycerides with ezetimibe and fenofibrate along with the citrus bergamot. I'm a fan of Cardarine, but there is no evidence that its effect on lipids is either beneficial or detrimental that I have found.
High-dose niacin is liver toxic and can increase insulin resistance.
Intuition can inform decisions, but it is no replacement for addressing health issues logically and methodically. But you do you.
High-dose niacin is liver toxic and can increase insulin resistance.
Intuition can inform decisions, but it is no replacement for addressing health issues logically and methodically. But you do you.
anon55
Member

I’m on 5mg Rosuvastatin and 10mg Ezetimibe. I consume roughly 60g of fiber daily (powerful and underrated way to reduce LDL as well).
Recent LDL: 25
I haven’t had ApoB checked in about a year but it was around 40 and might even be less now if I had to guess.
OTC supplements like citrus bergamot really don’t produce a dramatic enough effect and cost a lot more anyway. Not to mention there are no outcome studies on humans showing reduced mortality or cardiovascular events on supplements that mildly reduce LDL
Recent LDL: 25
I haven’t had ApoB checked in about a year but it was around 40 and might even be less now if I had to guess.
OTC supplements like citrus bergamot really don’t produce a dramatic enough effect and cost a lot more anyway. Not to mention there are no outcome studies on humans showing reduced mortality or cardiovascular events on supplements that mildly reduce LDL
egruberman
Member
uess my body doesn't work like the people in those trials. When I take the supplements I mentioned, I feel great, when I don't, I feel worse. Everyone's body is different, reading your body is what it all comes down to in the end.
Ultimately, I expect that you and everyone else make the best decision they can about their individual circumstances regardless of whether I agree with the approach.
The data I offer is based on a population and applies to a population. It represents the best evidence that I’m aware of, but it doesn’t give individual guidance. As AAS users we are all aware that our bodies react differently to various compounds. So, you do you.
I would, however encourage you to check out some of the latest data on niacin. It does improve lipids, but in spite of that, may be harmful.
The guidance I’ve offered will lower lipids, but more importantly, there is evidence of improved outcomes for each compound.
Citrus Bergamot reduced my LDL from 150 to 90 in 30 days.
Ezetimibe is kinda expensive here where I live, would you guys recommend running Rosuvastatin alone to control LDL? 5mg pills are dirt cheap here in the middle east straight from the pharmacy.
Ezetimibe is kinda expensive here where I live, would you guys recommend running Rosuvastatin alone to control LDL? 5mg pills are dirt cheap here in the middle east straight from the pharmacy.
egruberman
Member
Ezetimibe is kinda expensive here where I live, would you guys recommend running Rosuvastatin alone to control LDL? 5mg pills are dirt cheap here in the middle east straight from the pharmacy.
In terms of lipid lowering, Rosuvastatin is superior to most everything else. 2.5mg or 5mg will probably yield a 2x or 3x LDL reduction over ezetimibe mono therapy.
FWIW, ezetimibe and bempedoic acid are available from Indian Pharma very cheaply.
Sicsemptyran
Member
Just as you might find a random case study interesting. My own baseline natural LDL (ApoB to match) was around 200 first time I checked it, luckily very young when I did so. Completely overhauled the diet almost to an unsustainable level, LDL got down to 185. Genetic tests all negative, just some unknown genetic lottery I won.In terms of lipid lowering, Rosuvastatin is superior to most everything else. 2.5mg or 5mg will probably yield a 2x or 3x LDL reduction over ezetimibe mono therapy.
FWIW, ezetimibe and bempedoic acid are available from Indian Pharma very cheaply.
Decided to just give ezetimibe a go for giggles, assuming I’d need to throw on a couple other agents immediately. 10mg daily dropped my LDL to 100 and had maintained that.
Just began bempedoic acid and will see what that does, hoping for another hyper response but doubt I will get it! Interesting though that clearly my body was doing some sort of pathologic reabsorption of cholesterol and ezetimibe on its own nearly halved both my LDL and ApoB.
BamaCrazy
New Member
I’m taking 10mg/10mg of Rosuvastatin/Ezetimibe. I’m getting labs Wednesday. I have at least 12 months worth of bempedoic acid 180mg. If my lipids justify it would you add 180 or can you split them?In terms of lipid lowering, Rosuvastatin is superior to most everything else. 2.5mg or 5mg will probably yield a 2x or 3x LDL reduction over ezetimibe mono therapy.
FWIW, ezetimibe and bempedoic acid are available from Indian Pharma very cheaply.
Georgetrenson
Member
Ironically I don't do tren, just used it in my username as a joke. I tried it for a week and then realized I can get the same job done with Anavar.Let me start off by saying if your anti statin because of sides, but have done tren your opinion is not qualified for and intelligent conversation
Also didn't say I was anti statin, my main point was that other alternatives should be explored first, before using statins as a last resort.
Don't be too quick to make assumptions.
Georgetrenson
Member
I think this boils down to the flush vs flush free products. I've only taken Niacin w/ flushing, have had no liver or insulin sensitivity issues;I would, however encourage you to check out some of the latest data on niacin. It does improve lipids, but in spite of that, may be harmful.
I think these two products get mixed up and the entire supplement gets a bad rap due to the mixup
Sicsemptyran
Member
Niacin has been extensively studied. At best it does nothing for cardiovascular disease risk, and more recent data has shown that it may cause harm, despite raising HDL. This is similar to early drugs for cholesterol which dramatically raised HDL but actually started killing people and were taken off the market.I think this boils down to the flush vs flush free products. I've only taken Niacin w/ flushing, have had no liver or insulin sensitivity issues;
I think these two products get mixed up and the entire supplement gets a bad rap due to the mixup
That sort of thing is fairly common medicine. People who are dying of cancer oftentimes have low cholesterol, doesn’t mean having cancer is good for your mortality.
Then why is ezetimibe superior (it seems so from most replies on here)? Do you mind explaining? I'm not at all educated when it comes to cholesterol medications.In terms of lipid lowering, Rosuvastatin is superior to most everything else. 2.5mg or 5mg will probably yield a 2x or 3x LDL reduction over ezetimibe mono therapy.
FWIW, ezetimibe and bempedoic acid are available from Indian Pharma very cheaply.
SenorSuperdrol
Member
Idk who you are so why are you assuming I’m replying to you. My statement is to the entire idiotic community that would do tren and demonize a statin.Ironically I don't do tren, just used it in my username as a joke. I tried it for a week and then realized I can get the same job done with Anavar.
Also didn't say I was anti statin, my main point was that other alternatives should be explored first, before using statins as a last resort.
Don't be too quick to make assumptions.
Pharmaceuticals should be the first resort.
Once the endothelial glycocalyx is damaged you will have plaque build up, end of story. So eliminate as many of the variables as you can. IE- lipids, BP, inflammation (a whole other topic)
Im not playing games with atherosclerosis to try some bologna concoction of 17 herbs and spices.
Similar threads
- Replies
- 7
- Views
- 370
- Replies
- 3
- Views
- 157