Part 2 of Peter Bond's series on blood pressure is online now.
@PeterBond: "Having an increased blood pressure for a transient period of time isn’t particularly so problematic, however, a lot of anabolic steroid users tend to use anabolic steroids for years. Then it’s a different story. In this article I will lay out how you can monitor your blood pressure, when it’s wise to start treating it, and how you can potentially treat it."
 thinksteroids.com
thinksteroids.com
@PeterBond: "Having an increased blood pressure for a transient period of time isn’t particularly so problematic, however, a lot of anabolic steroid users tend to use anabolic steroids for years. Then it’s a different story. In this article I will lay out how you can monitor your blood pressure, when it’s wise to start treating it, and how you can potentially treat it."
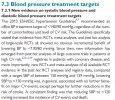
Measuring and Treating High Blood Pressure in Anabolic Steroid Users
In my previous article I discussed how there’s an increased mortality and morbidity risk when systolic blood pressure increases beyond 115 mmHg and
thinksteroids.com