How long can high dose GH be safely ran for, considering A1C and BG measurements are all in a healthy range? Is there anything worth considering from a risk assessment/health management standpoint? I’ve been playing with 15-20iu’s post workout for two months now and the only side I’ve recently developed is some CTS issues at night. A1C is under 5 and BG is below 80’s while bulking
@Type-IIx
As
@29trt intimated, the use of exogenous insulin
worsens systemic insulin sensitivity despite lowering blood glucose, because systemic insulin resistance is a product of blood insulin × glucose (HOMA-IR).
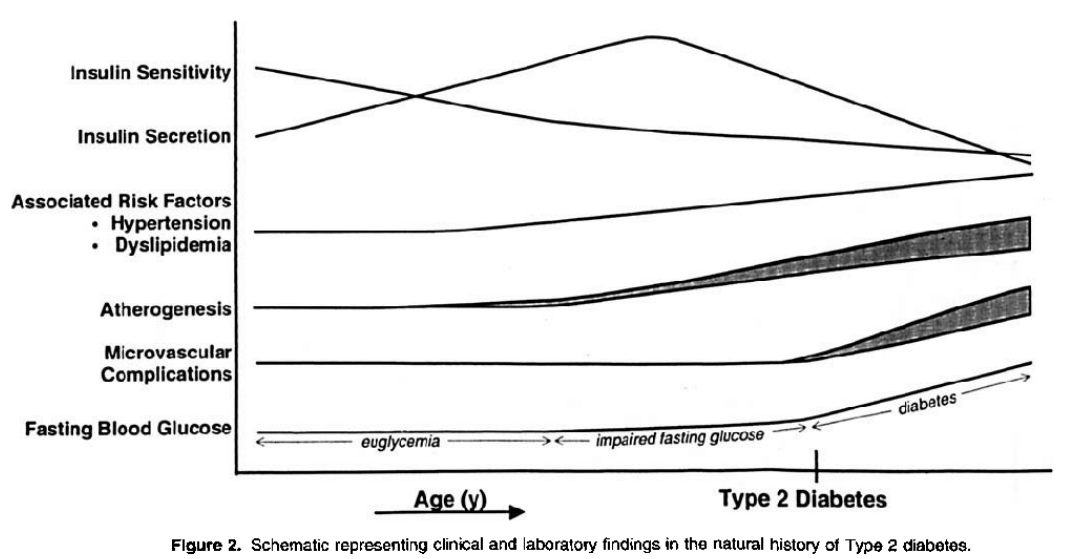
Hyperglycemia ≠ Insulin Resistance. Rather, the two are
associated in the pathogenesis or natural progression to T2DM. Note that elevated insulin secretion, reciprocal to insulin sensitivity, precedes elevations to blood glucose in this progression; and AAS promote the associated risk factors, as does insulin:
Glucotoxicity refers to the toxic effect that elevated glucose levels have, damaging the pancreatic β cells.
Regulation of insulin sensitivity occurs by several mechanisms – broadly,
central mechanisms include GLP-1 & GIP receptors;
peripheral mechanisms include transporter proteins, e.g. glucose transporters (e.g., GLUT-4 in skeletal muscle). HOMA-IR is one measure that provides insight into systemic insulin sensitivity (quantifying its reciprocal, insulin resistance).
You can read more about this & its mechanisms in the following article under the heading "Exogenous insulin-induced insulin resistance":
This article is intended to provide a comprehensive understanding on insulin actions for the bodybuilder and biochemist alike to counter a narrative that insulin is (supposedly) not muscle protein anabolic.

thinksteroids.com