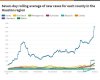
Latest #COVID19 for Harris County, my observations if this trajectory persists: 1) Houston would become the worst affected city in the US, maybe rival what we're seeing now in Brazil 2) The masks = good 1st step but simply won't be enough 3) We would need to proceed to red alert.
MESO-Rx
Anabolic Steroids
Navigation
Install the app
How to install the app on iOS
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
More options
Style variation
Guest viewing limit reached
- You have reached the maximum number of guest views allowed
- Please register below to remove this limitation
- Already a member? Click here to login
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Can touching a barbell in the gym get you sick with the coronavirus?
- Thread starter Michael Scally MD
- Start date
MisterSuperGod
New Member
For the second consecutive day, Florida announced a record number of new coronavirus cases Friday, adding almost 4,000 reports for a total approaching 90,000.
That broke the previous record set just Thursday, when 3,207 reports were added, according to the state Health Department.
Look's like it's time to...

That broke the previous record set just Thursday, when 3,207 reports were added, according to the state Health Department.
Look's like it's time to...
Around memorial day weekend, I got sick. Went to the ER after a week. Had bacterial pneumonia confirmed by a small lobe infiltrate and however else they determine it. Was put on zithromax for 5 days. No relief. Then did a round of doxycycline and just finished up this dexamethasone treatment. I still feel like shit in my 4th week of this. 2 negative covid tests. If I did catch the virus, I dont think I could physically handle any stronger meds. My gut feels like its blown out. I cant eat much but when I do...I'm just nauseous. Acid reflux constantly etc.Low-cost dexamethasone reduces death by up to one third in hospitalised patients with severe respiratory complications of COVID-19
16 June 2020
Statement from the Chief Investigators of the Randomised Evaluation of COVid-19 thERapY (RECOVERY) Trial on dexamethasone, 16 June 2020
In March 2020, the RECOVERY (Randomised Evaluation of COVid-19 thERapY) trial was established as a randomised clinical trial to test a range of potential treatments for COVID-19, including low-dose dexamethasone (a steroid treatment). Over 11,500 patients have been enrolled from over 175 NHS hospitals in the UK.
On 8 June, recruitment to the dexamethasone arm was halted since, in the view of the trial Steering Committee, sufficient patients had been enrolled to establish whether or not the drug had a meaningful benefit.
A total of 2104 patients were randomised to receive dexamethasone 6 mg once per day (either by mouth or by intravenous injection) for ten days and were compared with 4321 patients randomised to usual care alone. Among the patients who received usual care alone, 28-day mortality was highest in those who required ventilation (41%), intermediate in those patients who required oxygen only (25%), and lowest among those who did not require any respiratory intervention (13%).
Dexamethasone reduced deaths by one-third in ventilated patients (rate ratio 0.65 [95% confidence interval 0.48 to 0.88]; p=0.0003) and by one fifth in other patients receiving oxygen only (0.80 [0.67 to 0.96]; p=0.0021). There was no benefit among those patients who did not require respiratory support (1.22 [0.86 to 1.75]; p=0.14).
Based on these results, 1 death would be prevented by treatment of around 8 ventilated patients or around 25 patients requiring oxygen alone.
Given the public health importance of these results, we are now working to publish the full details as soon as possible.
Peter Horby, Professor of Emerging Infectious Diseases in the Nuffield Department of Medicine, University of Oxford, and one of the Chief Investigators for the trial, said: ‘Dexamethasone is the first drug to be shown to improve survival in COVID-19. This is an extremely welcome result. The survival benefit is clear and large in those patients who are sick enough to require oxygen treatment, so dexamethasone should now become standard of care in these patients. Dexamethasone is inexpensive, on the shelf, and can be used immediately to save lives worldwide.’
Martin Landray, Professor of Medicine and Epidemiology at the Nuffield Department of Population Health, University of Oxford, one of the Chief Investigators, said: ‘Since the appearance of COVID-19 six months ago, the search has been on for treatments that can improve survival, particularly in the sickest patients. These preliminary results from the RECOVERY trial are very clear – dexamethasone reduces the risk of death among patients with severe respiratory complications. COVID-19 is a global disease – it is fantastic that the first treatment demonstrated to reduce mortality is one that is instantly available and affordable worldwide.’
The UK Government’s Chief Scientific Adviser, Sir Patrick Vallance, said: ‘This is tremendous news today from the Recovery trial showing that dexamethasone is the first drug to reduce mortality from COVID-19. It is particularly exciting as this is an inexpensive widely available medicine.
‘This is a ground-breaking development in our fight against the disease, and the speed at which researchers have progressed finding an effective treatment is truly remarkable. It shows the importance of doing high quality clinical trials and basing decisions on the results of those trials.’
Notes
For interview requests, please contact: Genevieve Juillet, Media Relations Manager (Research and Innovation), University of Oxford.
Full details of the study protocol and related materials are available at www.recoverytrial.net.
A range of potential treatments have been suggested for COVID-19 but it has been unclear whether any of them will turn out to be more effective in improving survival than the usual standard of hospital care which all patients will receive.
About the RECOVERY trial
The RECOVERY trial is a large, randomised controlled trial of possible treatments for patients admitted to hospital with COVID-19. Over 11,500 patients have been randomised to the following treatment arms, or no additional treatment:
Overall dexamethasone reduced the 28-day mortality rate by 17% (0.83 [0.74 to 0.92]; P=0.0007) with a highly significant trend showing greatest benefit among those patients requiring ventilation (test for trend p<0.001). But it is important to recognise that we found no evidence of benefit for patients who did not require oxygen and we did not study patients outside the hospital setting. Follow-up is complete for over 94% of participants.
- Lopinavir-Ritonavir (commonly used to treat HIV)
- Low-dose Dexamethasone (a type of steroid, which typically used to reduce inflammation)
- Hydroxychloroquine (which has now been stopped due to lack of efficacy)
- Azithromycin (a commonly used antibiotic)
- Tocilizumab (an anti-inflammatory treatment given by injection)
- Convalescent plasma (collected from donors who have recovered from COVID-19 and contains antibodies against the SARS-CoV-2 virus).
The RECOVERY Trial is conducted by the registered clinical trials units with the Nuffield Department of Population Health in partnership with the Nuffield Department of Medicine. The trial is supported by a grant to the University of Oxford from UK Research and Innovation/National Institute for Health Research (NIHR) and by core funding provided by NIHR Oxford Biomedical Research Centre, Wellcome, the Bill and Melinda Gates Foundation, the Department for International Development, Health Data Research UK, the Medical Research Council Population Health Research Unit, and NIHR Clinical Trials Unit Support Funding.
The RECOVERY trial involves many thousands of doctors, nurses, pharmacists, and research administrators at over 175 hospitals across the whole of the UK, supported by staff at the NIHR Clinical Research Network, NHS DigiTrials, Public Health England, Public Health Scotland, Department of Health & Social Care, and the NHS in England, Scotland, Wales and Northern Ireland.
Source: Low-cost dexamethasone reduces death by up to one third in hospitalised patients with severe respiratory complications of COVID-19 — RECOVERY Trial
Low-cost dexamethasone reduces death by up to one third in hospitalised patients with severe respiratory complications of COVID-19
16 June 2020
Statement from the Chief Investigators of the Randomised Evaluation of COVid-19 thERapY (RECOVERY) Trial on dexamethasone, 16 June 2020
In March 2020, the RECOVERY (Randomised Evaluation of COVid-19 thERapY) trial was established as a randomised clinical trial to test a range of potential treatments for COVID-19, including low-dose dexamethasone (a steroid treatment). Over 11,500 patients have been enrolled from over 175 NHS hospitals in the UK.
On 8 June, recruitment to the dexamethasone arm was halted since, in the view of the trial Steering Committee, sufficient patients had been enrolled to establish whether or not the drug had a meaningful benefit.
A total of 2104 patients were randomised to receive dexamethasone 6 mg once per day (either by mouth or by intravenous injection) for ten days and were compared with 4321 patients randomised to usual care alone. Among the patients who received usual care alone, 28-day mortality was highest in those who required ventilation (41%), intermediate in those patients who required oxygen only (25%), and lowest among those who did not require any respiratory intervention (13%).
Dexamethasone reduced deaths by one-third in ventilated patients (rate ratio 0.65 [95% confidence interval 0.48 to 0.88]; p=0.0003) and by one fifth in other patients receiving oxygen only (0.80 [0.67 to 0.96]; p=0.0021). There was no benefit among those patients who did not require respiratory support (1.22 [0.86 to 1.75]; p=0.14).
Based on these results, 1 death would be prevented by treatment of around 8 ventilated patients or around 25 patients requiring oxygen alone.
Given the public health importance of these results, we are now working to publish the full details as soon as possible.
Peter Horby, Professor of Emerging Infectious Diseases in the Nuffield Department of Medicine, University of Oxford, and one of the Chief Investigators for the trial, said: ‘Dexamethasone is the first drug to be shown to improve survival in COVID-19. This is an extremely welcome result. The survival benefit is clear and large in those patients who are sick enough to require oxygen treatment, so dexamethasone should now become standard of care in these patients. Dexamethasone is inexpensive, on the shelf, and can be used immediately to save lives worldwide.’
Martin Landray, Professor of Medicine and Epidemiology at the Nuffield Department of Population Health, University of Oxford, one of the Chief Investigators, said: ‘Since the appearance of COVID-19 six months ago, the search has been on for treatments that can improve survival, particularly in the sickest patients. These preliminary results from the RECOVERY trial are very clear – dexamethasone reduces the risk of death among patients with severe respiratory complications. COVID-19 is a global disease – it is fantastic that the first treatment demonstrated to reduce mortality is one that is instantly available and affordable worldwide.’
The UK Government’s Chief Scientific Adviser, Sir Patrick Vallance, said: ‘This is tremendous news today from the Recovery trial showing that dexamethasone is the first drug to reduce mortality from COVID-19. It is particularly exciting as this is an inexpensive widely available medicine.
‘This is a ground-breaking development in our fight against the disease, and the speed at which researchers have progressed finding an effective treatment is truly remarkable. It shows the importance of doing high quality clinical trials and basing decisions on the results of those trials.’
Notes
For interview requests, please contact: Genevieve Juillet, Media Relations Manager (Research and Innovation), University of Oxford.
Full details of the study protocol and related materials are available at www.recoverytrial.net.
A range of potential treatments have been suggested for COVID-19 but it has been unclear whether any of them will turn out to be more effective in improving survival than the usual standard of hospital care which all patients will receive.
About the RECOVERY trial
The RECOVERY trial is a large, randomised controlled trial of possible treatments for patients admitted to hospital with COVID-19. Over 11,500 patients have been randomised to the following treatment arms, or no additional treatment:
Overall dexamethasone reduced the 28-day mortality rate by 17% (0.83 [0.74 to 0.92]; P=0.0007) with a highly significant trend showing greatest benefit among those patients requiring ventilation (test for trend p<0.001). But it is important to recognise that we found no evidence of benefit for patients who did not require oxygen and we did not study patients outside the hospital setting. Follow-up is complete for over 94% of participants.
- Lopinavir-Ritonavir (commonly used to treat HIV)
- Low-dose Dexamethasone (a type of steroid, which typically used to reduce inflammation)
- Hydroxychloroquine (which has now been stopped due to lack of efficacy)
- Azithromycin (a commonly used antibiotic)
- Tocilizumab (an anti-inflammatory treatment given by injection)
- Convalescent plasma (collected from donors who have recovered from COVID-19 and contains antibodies against the SARS-CoV-2 virus).
The RECOVERY Trial is conducted by the registered clinical trials units with the Nuffield Department of Population Health in partnership with the Nuffield Department of Medicine. The trial is supported by a grant to the University of Oxford from UK Research and Innovation/National Institute for Health Research (NIHR) and by core funding provided by NIHR Oxford Biomedical Research Centre, Wellcome, the Bill and Melinda Gates Foundation, the Department for International Development, Health Data Research UK, the Medical Research Council Population Health Research Unit, and NIHR Clinical Trials Unit Support Funding.
The RECOVERY trial involves many thousands of doctors, nurses, pharmacists, and research administrators at over 175 hospitals across the whole of the UK, supported by staff at the NIHR Clinical Research Network, NHS DigiTrials, Public Health England, Public Health Scotland, Department of Health & Social Care, and the NHS in England, Scotland, Wales and Northern Ireland.
Source: Low-cost dexamethasone reduces death by up to one third in hospitalised patients with severe respiratory complications of COVID-19 — RECOVERY Trial
Glucocorticoids as sepsis modulators has been debated for decades and COVID-19 is no exception.
Attachments
Latest #COVID19 for Harris County, my observations if this trajectory persists: 1) Houston would become the worst affected city in the US, maybe rival what we're seeing now in Brazil 2) The masks = good 1st step but simply won't be enough 3) We would need to proceed to red alert.
Another Red Alert pediatric pandemic panic based upon modeling IF's and exaggerated hospital occupancy rates blowing concerns from his ivory tower.
What did these "experts" anticipate once testing was accelerated, lower transmission rates, knowing protests that could fill Texans stadium will remain unchallanged and untouchable.
Find lot's of fire trucks, disable the Dow, fence the freeways, and gut the grocery stores.
There's a medical colloquialism that I try to live by -- ensure the treatment is not worse than the disease!
JIM
Last edited:
Theworm
Member
Quoting politico? Lol
Maybe we should all hide under our beds until Biden gets elected?
Citing Politico extensively quoting a Republican governor... Yeah, what da fuck's that about?! LolQuoting politico? Lol
Maybe we should all hide under our beds until Biden gets elected?
Theworm
Member
They always have a motive. Trump can cure cancer and they will criticize him for taking too long.Citing Politico extensively quoting a Republican governor... Yeah, what da fuck's that about?! Lol
Politico, riots don’t spread coronavirus but trump rallies do. Still haven’t figured that one out.
Theworm
Member
I really think most Americans aren’t buying into the fear mongering anymore. Most are taking precautions with distancing, masks, hygiene etc and understand there is a risk. But there’s also risks to flying, driving a car etc.
Most rational Americans are weighing the risks (maybe 20% chance or so in getting this, and about a 1% chance of dying), that’s about a .2 percent chance or less of dying. Most weigh the risk of that verse what the liberals want, total shut down, lock yourself in your house except to riot, (I mean “protest”), which would cost most lives. The huge recession/lockdown is causing more deaths and destruction than the virus (unemployment, bankruptcies, suicides, drug and alcohol abuse, domestic and child abuse on and on)... just look at the mike long lines at food banks, people are starving to death.
Most rational Americans are weighing the risks (maybe 20% chance or so in getting this, and about a 1% chance of dying), that’s about a .2 percent chance or less of dying. Most weigh the risk of that verse what the liberals want, total shut down, lock yourself in your house except to riot, (I mean “protest”), which would cost most lives. The huge recession/lockdown is causing more deaths and destruction than the virus (unemployment, bankruptcies, suicides, drug and alcohol abuse, domestic and child abuse on and on)... just look at the mike long lines at food banks, people are starving to death.
Theworm
Member
U.S. ‘deaths of despair’ from COVID-19 could top 75,000, experts warn
Publish date: May 8, 2020
Author(s):
Megan Brooks
An additional 75,000 Americans could die by suicide, drugs, or alcohol abuse because of the COVID-19 pandemic, projections from a new national report released today suggest.
The number of “deaths of despair” could be even higher if the country fails to take bold action to address the mental health toll of unemployment, isolation, and uncertainty, according to the report from the Well Being Trust (WBT) and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care.
“If nothing happens and nothing improves – ie, the worst-case scenario – we could be looking at an additional 150,000 people who died who didn’t have to,” Benjamin Miller, PsyD, WBT chief strategy officer, told Medscape Medical News.
Medscape.com.
Publish date: May 8, 2020
Author(s):
Megan Brooks
An additional 75,000 Americans could die by suicide, drugs, or alcohol abuse because of the COVID-19 pandemic, projections from a new national report released today suggest.
The number of “deaths of despair” could be even higher if the country fails to take bold action to address the mental health toll of unemployment, isolation, and uncertainty, according to the report from the Well Being Trust (WBT) and the Robert Graham Center for Policy Studies in Family Medicine and Primary Care.
“If nothing happens and nothing improves – ie, the worst-case scenario – we could be looking at an additional 150,000 people who died who didn’t have to,” Benjamin Miller, PsyD, WBT chief strategy officer, told Medscape Medical News.
Medscape.com.
Last edited:
SteroidsBro
New Member
4Figgy
New Member
I’m still confused as to why people are scared of this virus. It’s a virus, people will die, and this is life. Who’s willing to bet some money on the hype disappearing after November? Any takers......
Similar threads
- Replies
- 59
- Views
- 1K